

Withdrawal of Life-Sustaining Treatment Mediates Mortality in Patients With Intracerebral Hemorrhage With Impaired Consciousness
- PMID: 34583530
- PMCID: PMC8608746
- DOI: 10.1161/STROKEAHA.121.035233
Withdrawal of Life-Sustaining Treatment Mediates Mortality in Patients With Intracerebral Hemorrhage With Impaired Consciousness
Abstract
Background and purpose: Impaired level of consciousness (LOC) on presentation at hospital admission in patients with intracerebral hemorrhage (ICH) may affect outcomes and the decision to withhold or withdraw life-sustaining treatment (WOLST).
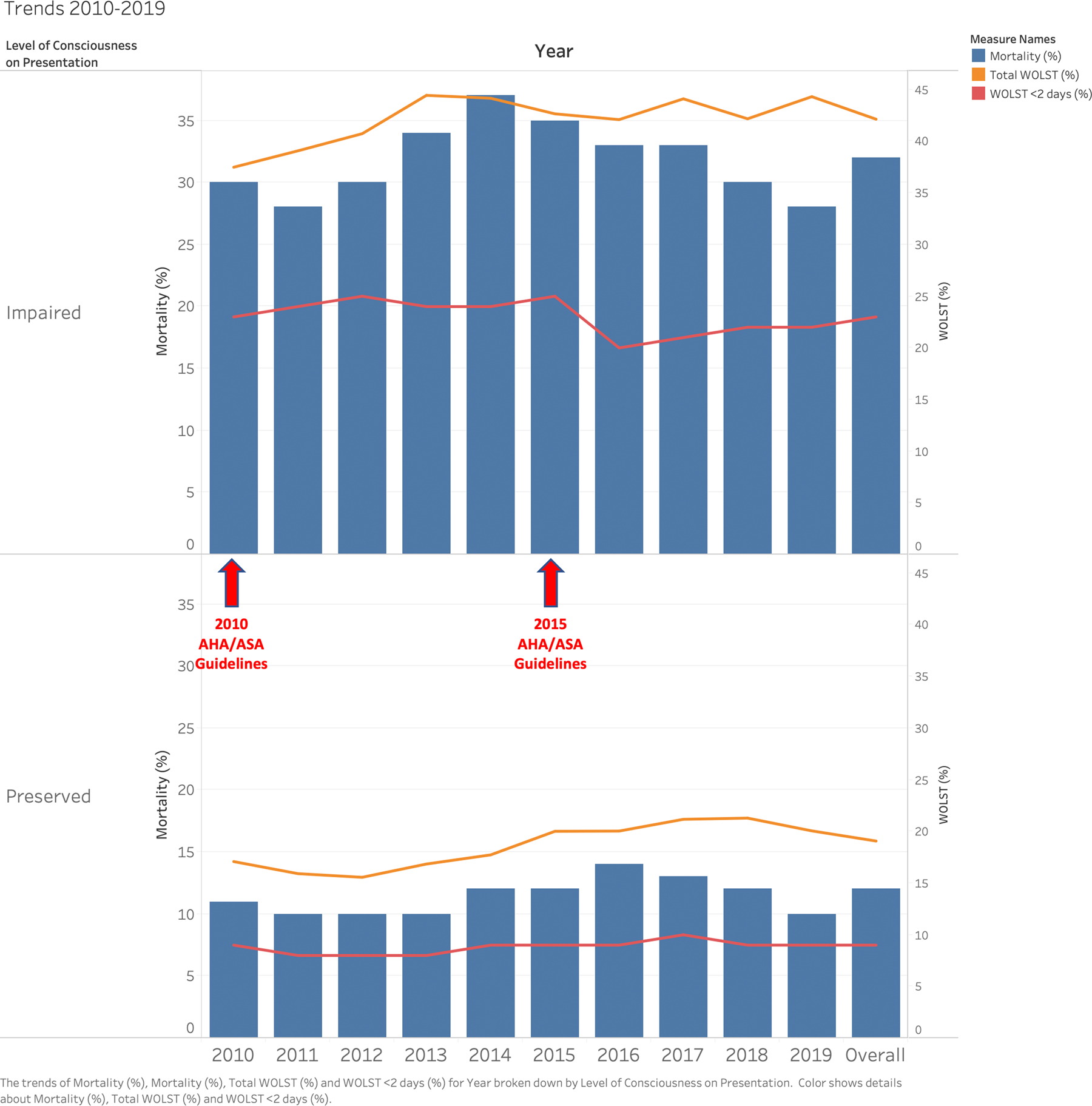
Methods: Patients with ICH were included across 121 Florida hospitals participating in the Florida Stroke Registry from 2010 to 2019. We studied the effect of LOC on presentation on in-hospital mortality (primary outcome), WOLST, ambulation status on discharge, hospital length of stay, and discharge disposition.
Results: Among 37 613 cases with ICH (mean age 71, 46% women, 61% White, 20% Black, 15% Hispanic), 12 272 (33%) had impaired LOC at onset. Compared with cases with preserved LOC, patients with impaired LOC were older (72 versus 70 years), more women (49% versus 45%), more likely to have aphasia (38% versus 16%), had greater ICH score (3 versus 1), greater risk of WOLST (41% versus 18%), and had an increased in-hospital mortality (32% versus 12%). In the multivariable-logistic regression with generalized estimating equations accounting for basic demographics, comorbidities, ICH severity, hospital size and teaching status, impaired LOC was associated with greater mortality (odds ratio, 3.7 [95% CI, 3.1-4.3], P<0.0001) and less likely discharged home or to rehab (odds ratio, 0.3 [95% CI, 0.3-0.4], P<0.0001). WOLST significantly mediated the effect of impaired LOC on mortality (mediation effect, 190 [95% CI, 152-229], P<0.0001). Early WOLST (<2 days) occurred among 51% of patients. A reduction in early WOLST was observed in patients with impaired LOC after the 2015 American Heart Association/American Stroke Association ICH guidelines recommending aggressive treatment and against early do-not-resuscitate.
Conclusions: In this large multicenter stroke registry, a third of ICH cases presented with impaired LOC. Impaired LOC was associated with greater in-hospital mortality and worse disposition at discharge, largely influenced by early decision to withhold or WOLST.
Keywords: aphasia; cerebral hemorrhage; consciousness; length of stay; logistic models.
Figures

Comment in
-
Future Shock: Does Pessimism Contribute to Poor Outcome After Intracerebral Hemorrhage?Stroke. 2021 Dec;52(12):3899-3900. doi: 10.1161/STROKEAHA.121.036761. Epub 2021 Sep 29. Stroke. 2021. PMID: 34583528 Free PMC article. No abstract available.
References
-
- Pinho J, Costa AS, Araújo JM, Amorim JM, Ferreira C. Intracerebral hemorrhage outcome: A comprehensive update. J Neurol Sci 2019;398:54–66 - PubMed
-
- Navarrete-Navarro P, Rivera-Fernández R, López-Mutuberría MT, Galindo I, Murillo F, Dominguez JM, et al. Outcome prediction in terms of functional disability and mortality at 1 year among icu-admitted severe stroke patients: A prospective epidemiological study in the south of the european union (evascan project, andalusia, spain). Intensive Care Med 2003;29:1237–1244 - PubMed
-
- Zahuranec DB, Brown DL, Lisabeth LD, Gonzales NR, Longwell PJ, Smith MA, et al. Early care limitations independently predict mortality after intracerebral hemorrhage. Neurology 2007;68:1651–1657 - PubMed
-
- Wabl R, Williamson CA, Pandey AS, Rajajee V. Long-term and delayed functional recovery in patients with severe cerebrovascular and traumatic brain injury requiring tracheostomy. J Neurosurg 2018;131:114–121 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
