

Facilitators and barriers to post-discharge pain assessment and triage: a qualitative study of nurses' and patients' perspectives
- PMID: 34583702
- PMCID: PMC8480104
- DOI: 10.1186/s12913-021-07031-w
Facilitators and barriers to post-discharge pain assessment and triage: a qualitative study of nurses' and patients' perspectives
Abstract
Background: After hospital discharge, patients can experience symptoms prompting them to seek acute medical attention. Early evaluation of patients' post-discharge symptoms by healthcare providers may improve appropriate healthcare utilization and patient safety. Post-discharge follow-up phone calls, which are used for routine transitional care in U.S. hospitals, serve as an important channel for provider-patient communication about symptoms. This study aimed to assess the facilitators and barriers to evaluating and triaging pain symptoms in cardiovascular patients through follow-up phone calls after their discharge from a large healthcare system in Central Massachusetts. We also discuss strategies that may help address the identified barriers.
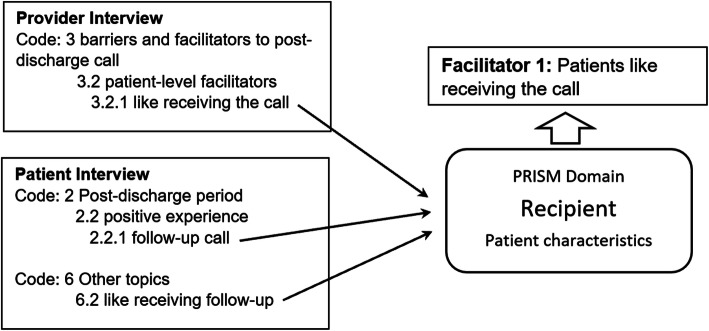
Methods: Guided by the Practical, Robust, Implementation and Sustainability Model (PRISM), we completed semi-structured interviews with 7 nurses and 16 patients in 2020. Selected nurses conducted (or supervised) post-discharge follow-up calls on behalf of 5 clinical teams (2 primary care; 3 cardiology). We used thematic analysis to identify themes from interviews and mapped them to the domains of the PRISM model.
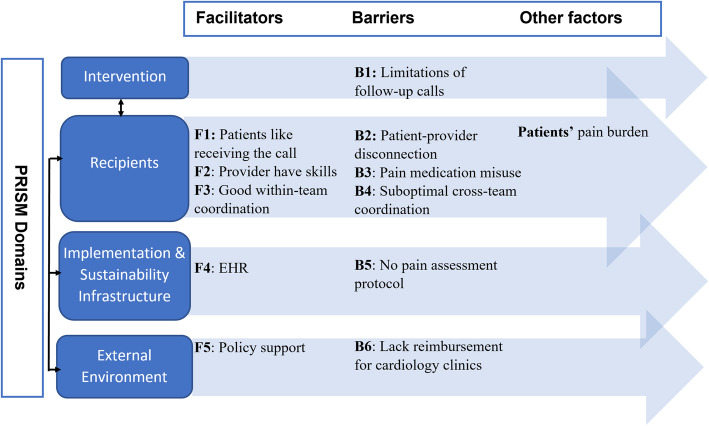
Results: Participants described common facilitators and barriers related to the four domains of PRISM: Intervention (I), Recipients (R), Implementation and Sustainability Infrastructure (ISI), and External Environment (EE). Facilitators include: (1) patients being willing to receive provider follow-up (R); (2) nurses experienced in symptom assessment (R); (3) good care coordination within individual clinical teams (R); (4) electronic health record system and call templates to support follow-up calls (ISI); and (5) national and institutional policies to support post-discharge follow-up (EE). Barriers include: (1) limitations of conducting symptom assessment by provider-initiated follow-up calls (I); (2) difficulty connecting patients and providers in a timely manner (R); (3) suboptimal coordination for transitional care among primary care and cardiology providers (R); and (4) lack of emphasis on post-discharge follow-up call reimbursement among cardiology clinics (EE). Specific barriers for pain assessment include: (1) concerns with pain medication misuse (R); and (2) no standardized pain assessment and triage protocol (ISI).
Conclusions: Strategies to empower patients, facilitate timely patient-provider communication, and support care coordination regarding pain evaluation and treatment may reduce the barriers and improve processes and outcomes of pain assessment and triage.
Keywords: Cardiovascular disease; Natural language processing; Pain; Qualitative; Symptom assessment; Transitional care.
© 2021. The Author(s).
Conflict of interest statement
Dr. McManus reports grants and personal fees from Bristol Myers Squibb, grants and personal fees from Pfizer, grants from Boehringer Ingelheim and Philips, non-financial support from Apple, personal fees and non-financial support from Samsung, grants and personal fees from Flexcon, personal fees from Avania, personal fees from Rose Consulting, grants and personal fees from Heart Rhythm Society, personal fees and non-financial support from Fitbit, outside the submitted work. The remaining authors have declared no competing interests.
Figures
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Shay CM, Spartano NL, Stokes A, Tirschwell DL, VanWagner L, Tsao CW, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi: 10.1161/CIR.0000000000000757. - DOI - PubMed
-
- Dharmarajan K, Hsieh AF, Lin Z, Bueno H, Ross JS, Horwitz LI, Barreto-Filho JA, Kim N, Bernheim SM, Suter LG, Drye EE, Krumholz HM. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355–363. doi: 10.1001/jama.2012.216476. - DOI - PMC - PubMed
-
- Iribarne A, Chang H, Alexander JH, Gillinov AM, Moquete E, Puskas JD, Bagiella E, Acker MA, Mayer ML, Ferguson TB, Burks S, Perrault LP, Welsh S, Johnston KC, Murphy M, DeRose JJ, Neill A, Dobrev E, Baio KT, Taddei-Peters W, Moskowitz AJ, O’Gara PT. Readmissions after cardiac surgery: experience of the National Institutes of Health/Canadian Institutes of Health research cardiothoracic surgical trials network. Ann Thorac Surg. 2014;98(4):1274–1280. doi: 10.1016/j.athoracsur.2014.06.059. - DOI - PMC - PubMed
-
- Kwok CS, Shah B, Al-Suwaidi J, Fischman DL, Holmvang L, Alraies C, et al. Timing and causes of unplanned readmissions after percutaneous coronary intervention: insights from the Nationwide readmission database. JACC Cardiovasc Interv. 2019;12(8):734–748. doi: 10.1016/j.jcin.2019.02.007. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
