

Performance of prediction models for nephropathy in people with type 2 diabetes: systematic review and external validation study
- PMID: 34583929
- PMCID: PMC8477272
- DOI: 10.1136/bmj.n2134
Performance of prediction models for nephropathy in people with type 2 diabetes: systematic review and external validation study
Abstract
Objectives: To identify and assess the quality and accuracy of prognostic models for nephropathy and to validate these models in external cohorts of people with type 2 diabetes.
Design: Systematic review and external validation.
Data sources: PubMed and Embase.
Eligibility criteria: Studies describing the development of a model to predict the risk of nephropathy, applicable to people with type 2 diabetes.
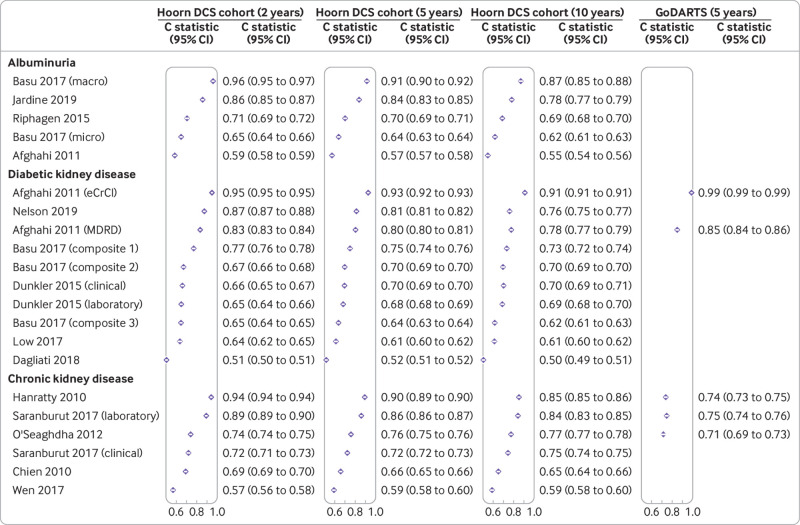
Methods: Screening, data extraction, and risk of bias assessment were done in duplicate. Eligible models were externally validated in the Hoorn Diabetes Care System (DCS) cohort (n=11 450) for the same outcomes for which they were developed. Risks of nephropathy were calculated and compared with observed risk over 2, 5, and 10 years of follow-up. Model performance was assessed based on intercept adjusted calibration and discrimination (Harrell's C statistic).
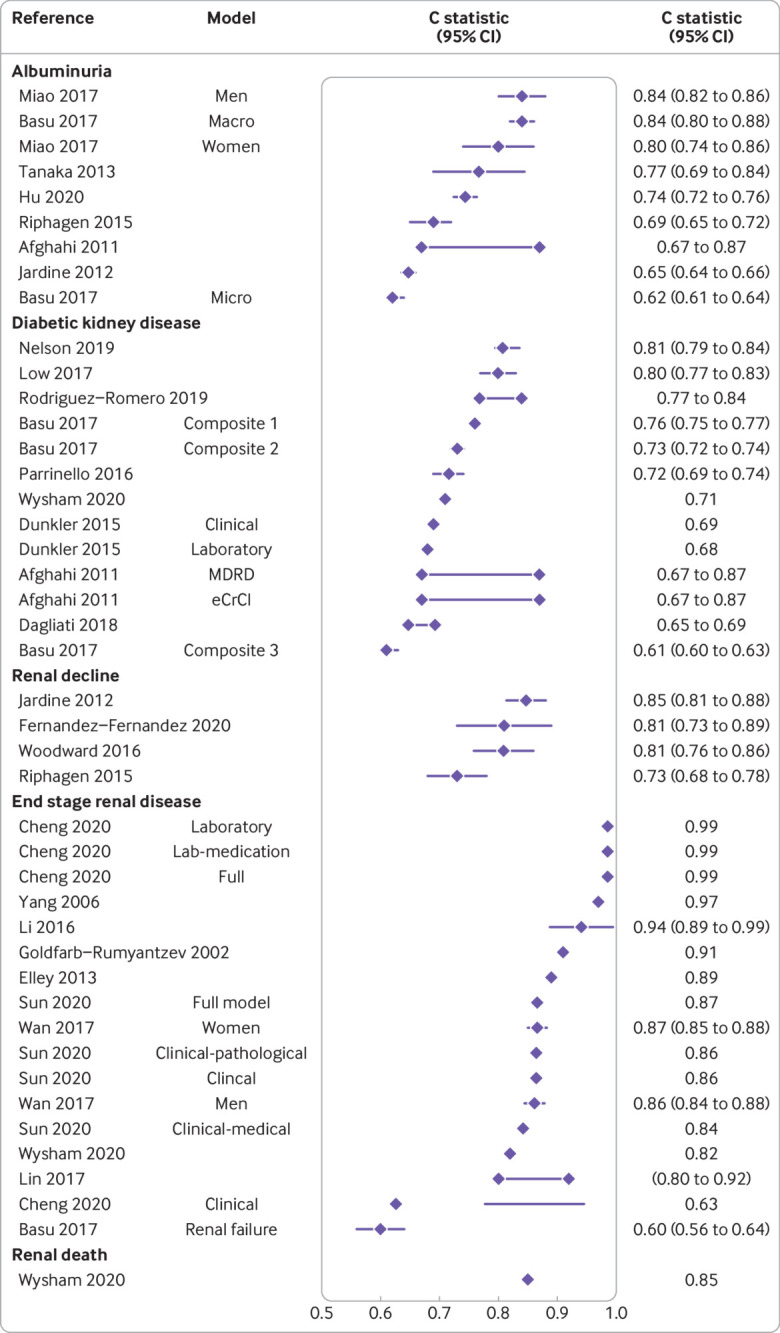
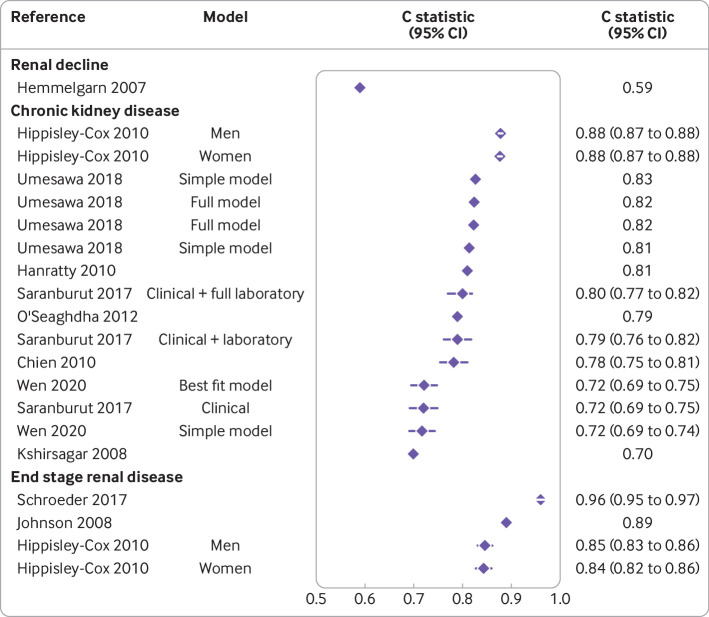
Results: 41 studies included in the systematic review reported 64 models, 46 of which were developed in a population with diabetes and 18 in the general population including diabetes as a predictor. The predicted outcomes included albuminuria, diabetic kidney disease, chronic kidney disease (general population), and end stage renal disease. The reported apparent discrimination of the 46 models varied considerably across the different predicted outcomes, from 0.60 (95% confidence interval 0.56 to 0.64) to 0.99 (not available) for the models developed in a diabetes population and from 0.59 (not available) to 0.96 (0.95 to 0.97) for the models developed in the general population. Calibration was reported in 31 of the 41 studies, and the models were generally well calibrated. 21 of the 64 retrieved models were externally validated in the Hoorn DCS cohort for predicting risk of albuminuria, diabetic kidney disease, and chronic kidney disease, with considerable variation in performance across prediction horizons and models. For all three outcomes, however, at least two models had C statistics >0.8, indicating excellent discrimination. In a secondary external validation in GoDARTS (Genetics of Diabetes Audit and Research in Tayside Scotland), models developed for diabetic kidney disease outperformed those for chronic kidney disease. Models were generally well calibrated across all three prediction horizons.
Conclusions: This study identified multiple prediction models to predict albuminuria, diabetic kidney disease, chronic kidney disease, and end stage renal disease. In the external validation, discrimination and calibration for albuminuria, diabetic kidney disease, and chronic kidney disease varied considerably across prediction horizons and models. For each outcome, however, specific models showed good discrimination and calibration across the three prediction horizons, with clinically accessible predictors, making them applicable in a clinical setting.
Systematic review registration: PROSPERO CRD42020192831.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from Dutch Diabetes Research foundation Fund, IMI-RHAPSODY, and ZorgInstitute Netherlands (Dutch Healthcare Institute) for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Federation ID. IDF Diabetes Atlas. 2015.
-
- Thomas S, Karalliede J. Diabetic nephropathy. Medicine (Baltimore) 2014;43:20-510.1016/j.mpmed.2014.10.007. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical