

Frequency of microsatellite instability (MSI) in upper tract urothelial carcinoma: comparison of the Bethesda panel and the Idylla MSI assay in a consecutively collected, multi-institutional cohort
- PMID: 34583948
- PMCID: PMC9887356
- DOI: 10.1136/jclinpath-2021-207855
Frequency of microsatellite instability (MSI) in upper tract urothelial carcinoma: comparison of the Bethesda panel and the Idylla MSI assay in a consecutively collected, multi-institutional cohort
Abstract
Aims: Upper tract urothelial carcinoma (UTUC) is a rare malignancy with a poor prognosis which occurs sporadically or in few cases results from a genetic disorder called Lynch syndrome. Recently, examination of microsatellite instability (MSI) has gained importance as a biomarker: MSI tumours are associated with a better response to immunomodulative therapies. Limited data are known about the prevalence of MSI in UTUC. New detection methods using the fully automated Idylla MSI Assay facilitate analysis of increased patient numbers.
Methods: We investigated the frequency of MSI in a multi-institutional cohort of 243 consecutively collected UTUC samples using standard methodology (Bethesda panel), along with immunohistochemistry of mismatch repair (MMR) proteins. The same tumour cohort was retested using the Idylla MSI Assay by Biocartis.
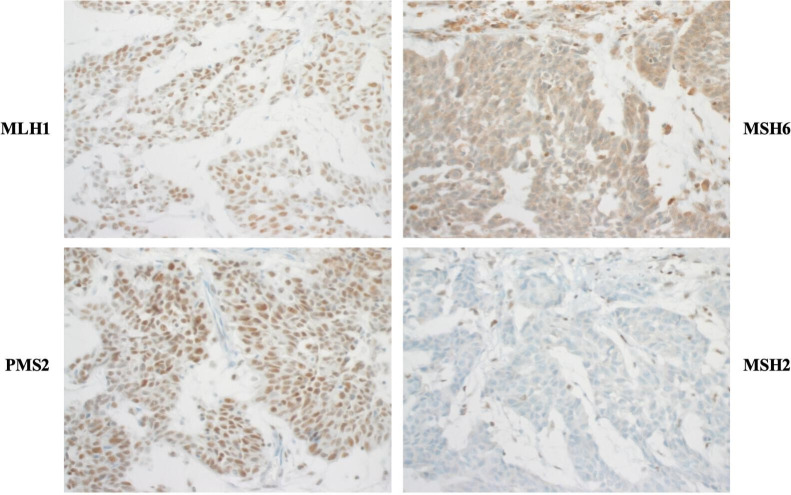
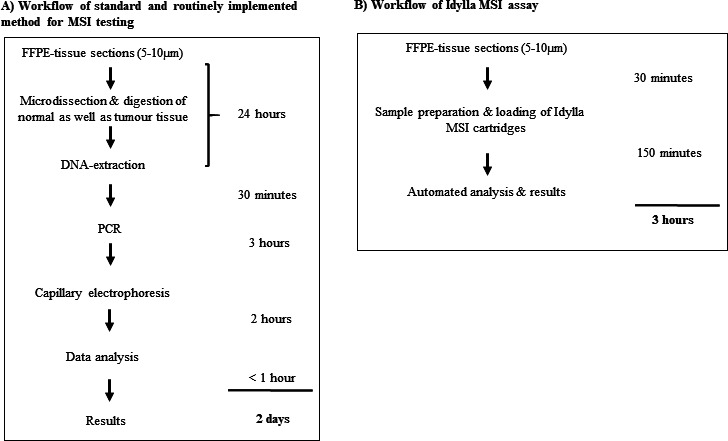
Results: Using standard methodology, 230/243 tumours were detected as microsatellite stable (MSS), 4/243 tumours as MSI and 9/243 samples as invalid. In comparison, the Idylla MSI Assay identified four additional tumours as MSS, equalling 234/243 tumours; 4/243 were classified as MSI and only 5/243 cases as invalid. At the immunohistochemical level, MSI results were supported in all available cases with a loss in MMR proteins. The overall concordance between the standard and the Idylla MSI Assay was 98.35%. Time to result differed between 3 hours for Idylla MSI Assay and 2 days with the standard methodology.
Conclusion: Our data indicate a low incidence rate of MSI tumours in patients with UTUC. Furthermore, our findings highlight that Idylla MSI Assay can be applied as an alternative method of MSI analysis for UTUC.
Keywords: methods; molecular; pathology; urological neoplasms.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Kohlmann W, Gruber SB, Syndrome L, eds. GeneReviews((R)). Seattle (WA), 1993.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical