

Health care costs associated with hepatitis C virus infection in First Nations populations in Ontario: a retrospective matched cohort study
- PMID: 34584004
- PMCID: PMC8486469
- DOI: 10.9778/cmajo.20200247
Health care costs associated with hepatitis C virus infection in First Nations populations in Ontario: a retrospective matched cohort study
Abstract
Background: Colonization and marginalization have affected the risk for and experience of hepatitis C virus (HCV) infection for First Nations people in Canada. In partnership with the Ontario First Nations HIV/AIDS Education Circle, we estimated the publicly borne health care costs associated with HCV infection among Status First Nations people in Ontario.
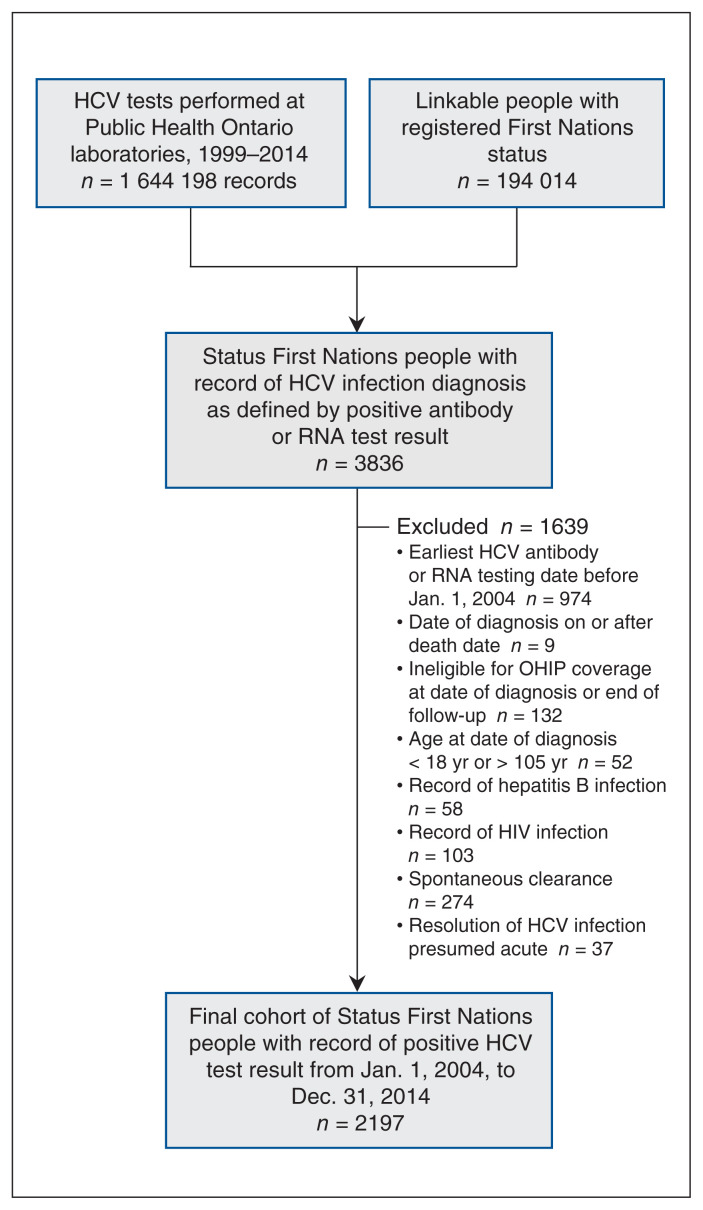
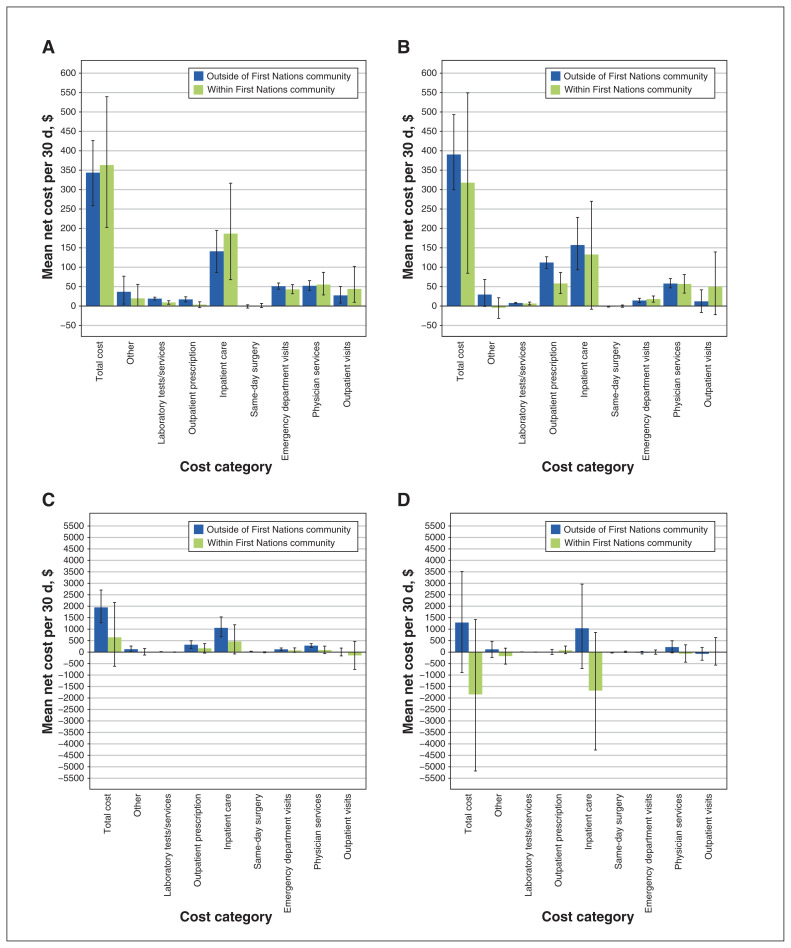
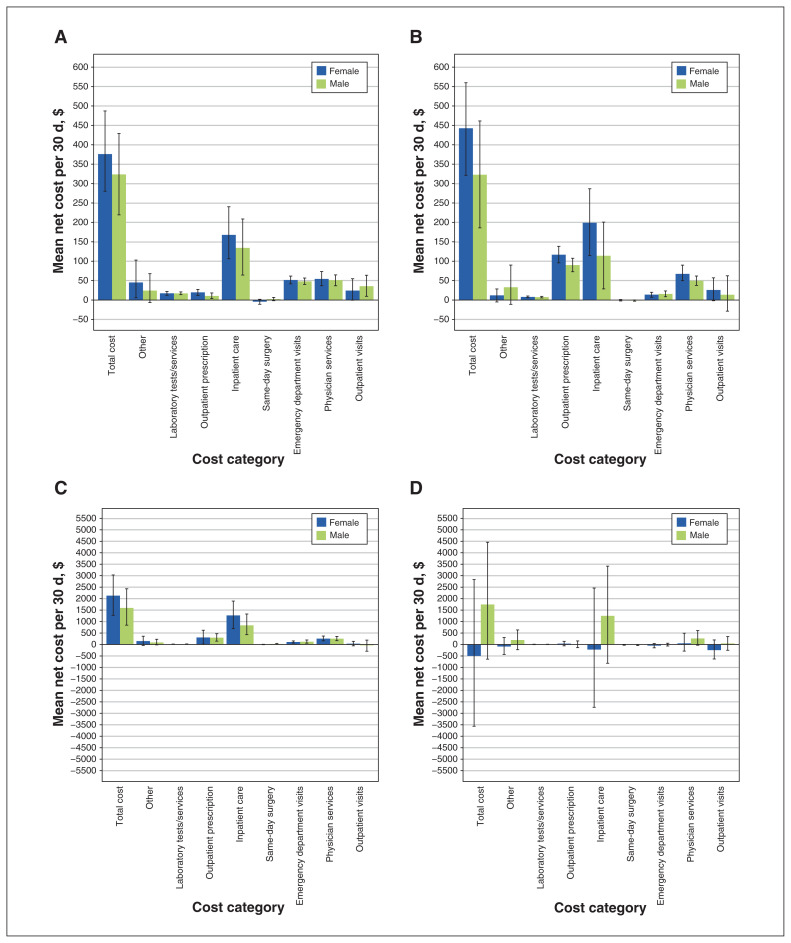
Methods: In this retrospective matched cohort study, we used linked health administrative databases to identify Status First Nations people in Ontario who tested positive for HCV antibodies or RNA between 2004 and 2014, and Status First Nations people who had no HCV testing records or only a negative test result (control group, matched 2:1 to case participants). We estimated total and net costs (difference between case and control participants) for 4 phases of care: prediagnosis (6 mo before HCV infection diagnosis), initial (after diagnosis), late (liver disease) and terminal (6 mo before death), until death or Dec. 31, 2017, whichever occurred first. We stratified costs by sex and residence within or outside of First Nations communities. All costs were measured in 2018 Canadian dollars.
Results: From 2004 to 2014, 2197 people were diagnosed with HCV infection. The mean net total costs per 30 days of HCV infection were $348 (95% confidence interval [CI] $277 to $427) for the prediagnosis phase, $377 (95% CI $288 to $470) for the initial phase, $1768 (95% CI $1153 to $2427) for the late phase and $893 (95% CI -$1114 to $3149) for the terminal phase. After diagnosis of HCV infection, net costs varied considerably among those who resided within compared to outside of First Nations communities. Net costs were higher for females than for males except in the terminal phase.
Interpretation: The costs per 30 days of HCV infection among Status First Nations people in Ontario increased substantially with progression to advanced liver disease and finally to death. These estimates will allow for planning and evaluation of provincial and territorial population-specific hepatitis C control efforts.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: William Wong and Murray Krahn report research support from the Canadian Liver Foundation. Jordan Feld reports institutional research support from AbbVie, Enanta Pharmaceuticals, Gilead Sciences and Janssen, and consulting fees from AbbVie and Gilead Sciences. No other competing interests were declared.
Figures
Comment in
-
Hepatitis C virus infection in First Nations populations in Ontario from 2006 to 2014: a population-based retrospective cohort analysis.CMAJ Open. 2021 Sep 28;9(3):E886-E896. doi: 10.9778/cmajo.20200164. Print 2021 Jul-Sep. CMAJ Open. 2021. PMID: 34584007 Free PMC article.
References
-
- Kwong JC, Crowcroft NS, Campitelli MA, et al. Ontario Burden of Infectious Disease Study Advisory Group. Ontario Burden of Infectious Disease Study (ONBOIDS): an OAHPP/ICES report. Toronto: Ontario Agency for Health Protection and Promotion, Institute for Clinical Evaluative Sciences; 2010.
-
- Kelly EM, James PD, Murthy S, et al. Health care utilization and costs for patients with end-stage liver disease are significantly higher at the end of life compared to those of other decedents. Clin Gastroenterol Hepatol. 2019;17:2339–46.e1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials