

Glial and myeloid heterogeneity in the brain tumour microenvironment
- PMID: 34584243
- PMCID: PMC8616823
- DOI: 10.1038/s41568-021-00397-3
Glial and myeloid heterogeneity in the brain tumour microenvironment
Abstract
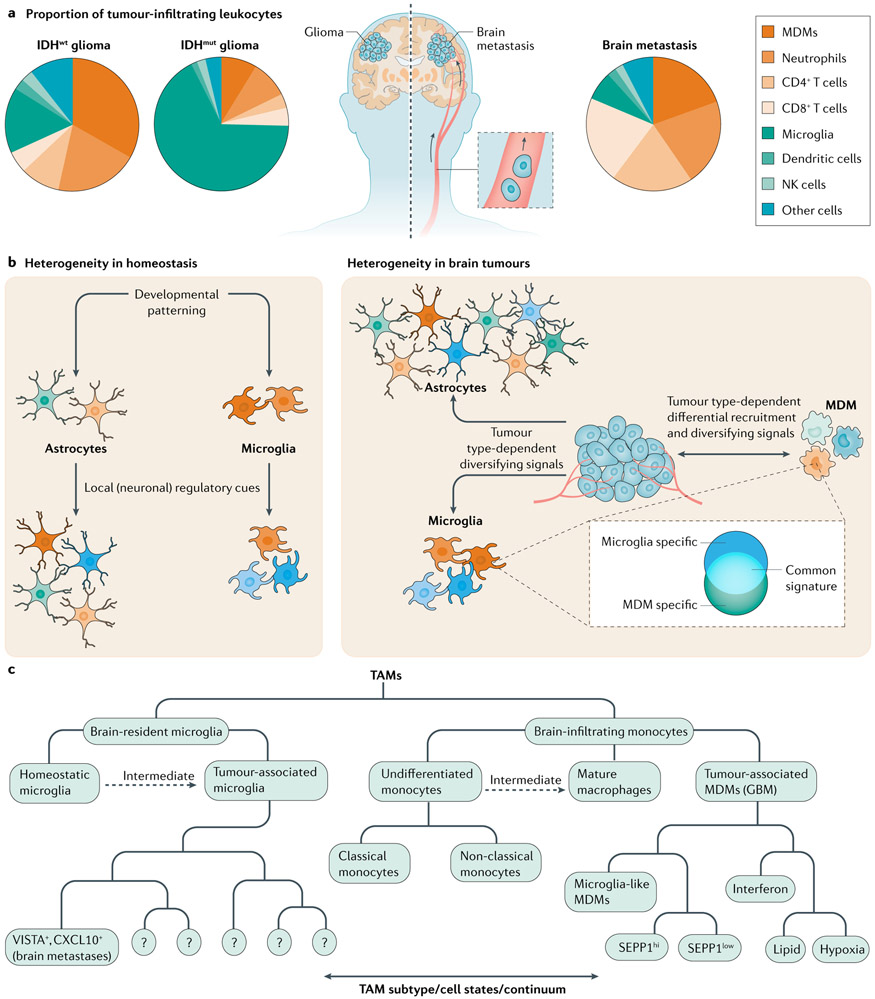
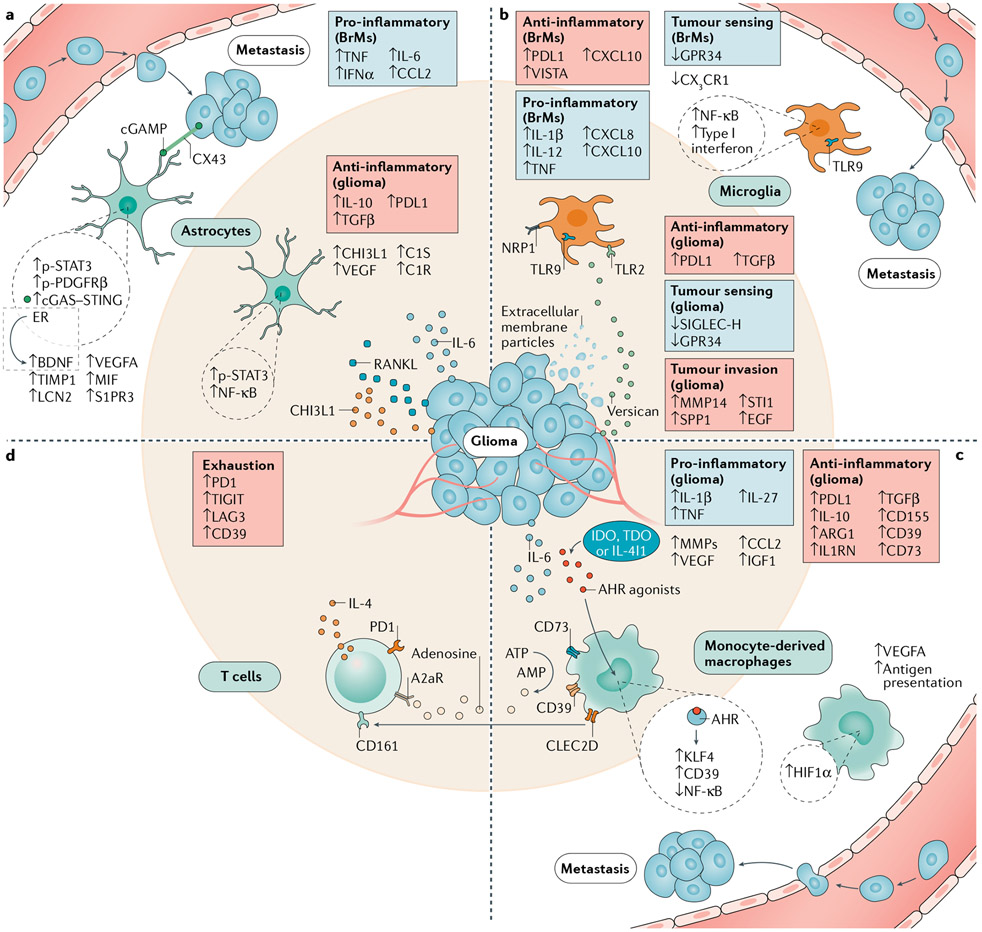
Brain cancers carry bleak prognoses, with therapeutic advances helping only a minority of patients over the past decade. The brain tumour microenvironment (TME) is highly immunosuppressive and differs from that of other malignancies as a result of the glial, neural and immune cell populations that constitute it. Until recently, the study of the brain TME was limited by the lack of methods to de-convolute this complex system at the single-cell level. However, novel technical approaches have begun to reveal the immunosuppressive and tumour-promoting properties of distinct glial and myeloid cell populations in the TME, identifying new therapeutic opportunities. Here, we discuss the immune modulatory functions of microglia, monocyte-derived macrophages and astrocytes in brain metastases and glioma, highlighting their disease-associated heterogeneity and drawing from the insights gained by studying these malignancies and other neurological disorders. Lastly, we consider potential approaches for the therapeutic modulation of the brain TME.
© 2021. Springer Nature Limited.
Figures
References
-
- Long GV et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: a multicentre randomised phase 2 study. Lancet Oncol. 19, 672–681 (2018). - PubMed
-
- Fecci PE et al. Increased regulatory T-cell fraction amidst a diminished CD4 compartment explains cellular immune defects in patients with malignant glioma. Cancer Res. 66, 3294–3302 (2006). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
