

Surgical mediastinal lymph node staging for non-small-cell lung carcinoma
- PMID: 34584863
- PMCID: PMC8435384
- DOI: 10.21037/tlcr-21-364
Surgical mediastinal lymph node staging for non-small-cell lung carcinoma
Abstract
Background: The current preferred approach for surgical mediastinal staging of non-small-cell lung carcinoma is video-assisted mediastinoscopy. An alternative technique in which lymph nodes are resected instead of biopsied is video-assisted mediastinoscopic lymphadenectomy (VAMLA) that is suggested to be superior in detecting N2 disease. Yet, evidence is conflicting and furthermore limited by sample size. The objective was to compare mediastinal staging through VAMLA and video-assisted mediastinoscopy.
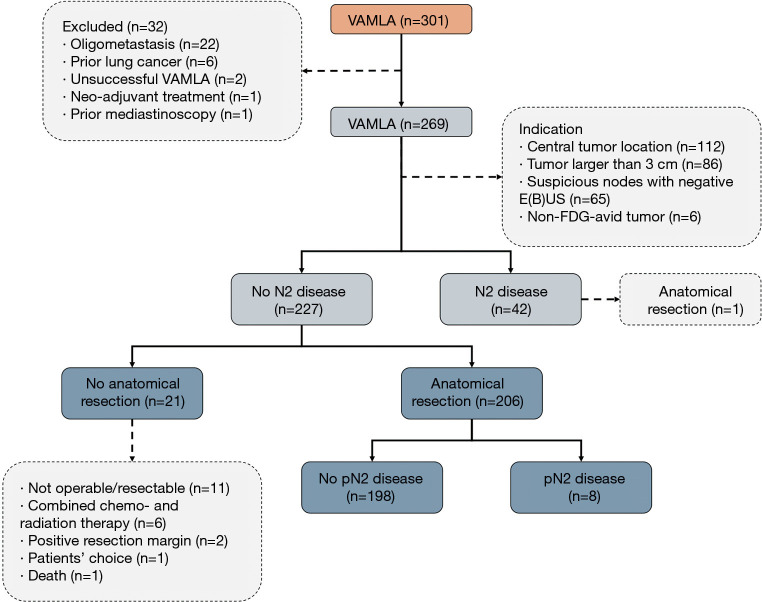
Methods: A single-center cohort study was conducted. All consecutive patients that underwent surgical mediastinal staging of non-small-cell lung carcinoma by VAMLA (2011 to 2018) were compared to historic video-assisted mediastinoscopy controls (2007 to 2011). Patients with negative surgical mediastinal staging underwent subsequent anatomical resection with systematic regional lymphadenectomy. Primary outcome was the sensitivity and negative predictive value for detecting N2 disease.
Results: Two-hundred-sixty-nine video-assisted mediastinoscopic lymphadenectomies and 118 video-assisted mediastinoscopies were performed. The prevalence of N2 disease was 20% and 26% respectively in the VAMLA and video-assisted mediastinoscopy group, while the rate of unforeseen pN2 resulting from lymph node dissection during anatomical resection was 4% and 11%, respectively. Invasive staging using VAMLA demonstrated superior sensitivity of 0.82 and a negative predictive value of 0.96 when compared to video-assisted mediastinoscopy (0.62 and 0.89, respectively), offering a 64% decrease in risk of unforeseen pN2 following anatomical resection. However, VAMLA is also associated with a 75% risk increase on complications (P=0.36).
Conclusions: We conclude that performing invasive mediastinal lymph node assessment for staging of non-small-cell lung carcinoma, VAMLA should be the preferred technique with superior sensitivity and negative predictive value in detecting N2 disease. Though, VAMLA is also associated with an increased risk of complications.
Keywords: Non-small cell lung carcinoma (NSCLC); sensitivity; unforeseen pN2 disease; video-assisted mediastinoscopic lymphadenectomy (VAMLA); video-assisted mediastinoscopy.
2021 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/tlcr-21-364). The authors have no conflicts of interest to declare.
Figures


References
-
- Silvestri GA, Gonzalez AV, Jantz MA, et al. Methods for staging non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e211S-e250S. - PubMed
LinkOut - more resources
Full Text Sources