

Placental abnormalities in congenital heart disease
- PMID: 34584887
- PMCID: PMC8429875
- DOI: 10.21037/tp-20-347
Placental abnormalities in congenital heart disease
Abstract
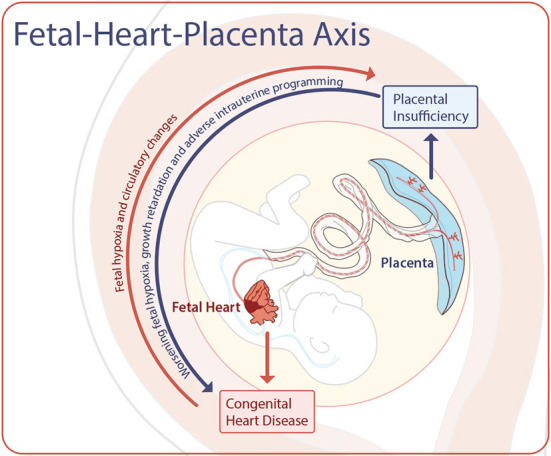
Congenital heart disease (CHD) remains the most common birth defect in infants, and critical CHD is associated with significant rates of morbidity and mortality. With the advent of powerful yet noninvasive advanced fetal imaging, it is becoming increasingly evident that the presence of CHD in utero disrupts typical development and contributes to the lifelong morbidity in this population. Across healthy and high-risk populations, intrauterine influences can permanently alter fetal development that may manifest in complex morbidities later in life, the so-called fetal-onset-of-adult-disease (FOAD) phenomenon. The placenta plays a critical role in not only supporting fetal development, but also by adapting to specific intrauterine conditions. The role of placental health, adaptation and dysfunction, however, in CHD is not well understood. In this article, we will review current evidence relating placental health in CHD, appraise existing knowledge-gaps in the field and highlight promising new avenues to better understand the impact of placental function on fetal well-being. We will review evidence of ex vivo human placental studies that describe abnormal placental findings in pregnancies complicated by CHD, as well evidence for in vivo assessments of the human placenta. While overall clinical in vivo assessments of placental development are rather limited, we will also review emerging evidence from advanced quantitative and functional magnetic resonance imaging that are bringing new insights into placental structure and function throughout gestation. By providing novel information about placental development, we can now explore the maternal-fetal-placental connection in greater detail, and better understand the multi-factorial mechanisms that may contribute to adverse outcomes seen in survivors of CHD.
Keywords: Placenta; congenital heart disease (CHD); imaging; magnetic resonance imaging; ultrasound.
2021 Translational Pediatrics. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tp-20-347). The series “Pre-natal Diagnosis in Congenital Heart Defects” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures
References
-
- Herrera E, Amusquivar E, Lopez-Soldado I, et al. Maternal lipid metabolism and placental lipid transfer. Horm Res 2006;65 Suppl 3:59-64. - PubMed
-
- Clifton VL, Read MA, Leitch IM, et al. Corticotropin-releasing hormone-induced vasodilatation in the human fetal placental circulation. J Clin Endocrinol Metab 1994;79:666-9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources