

Fetal brain issues in congenital heart disease
- PMID: 34584890
- PMCID: PMC8429876
- DOI: 10.21037/tp-20-224
Fetal brain issues in congenital heart disease
Abstract
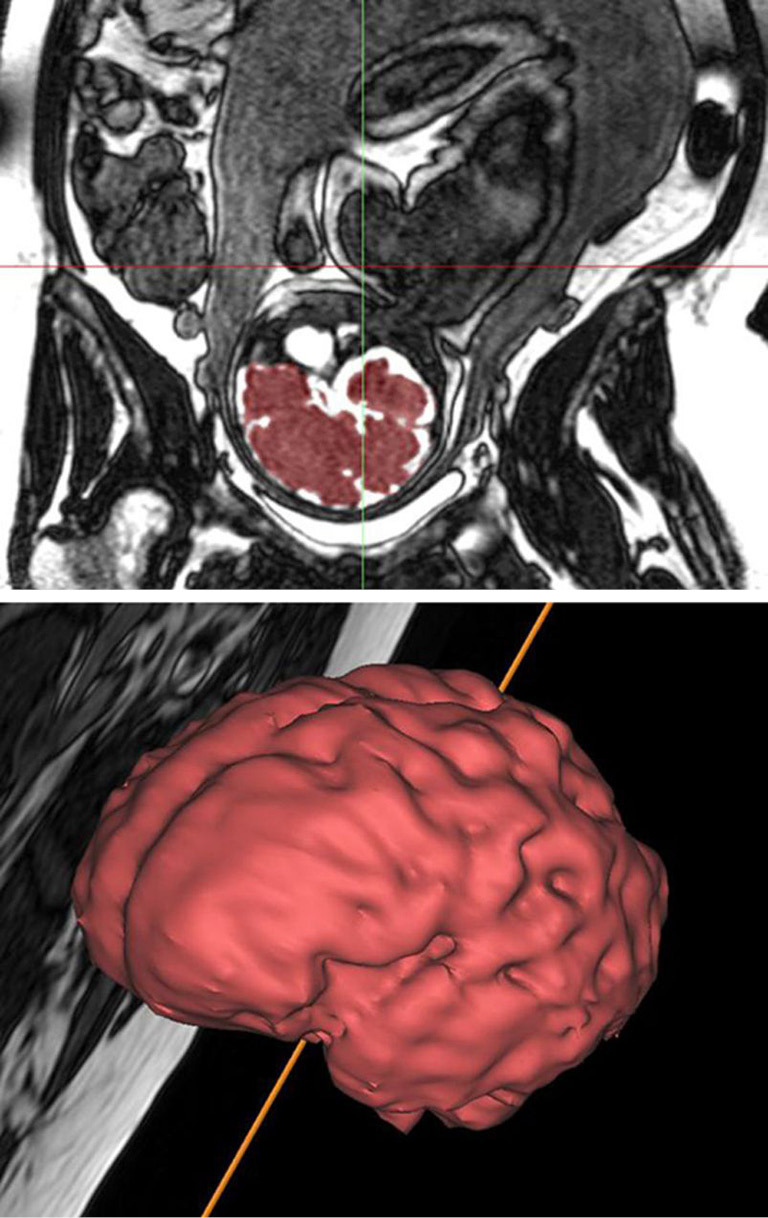
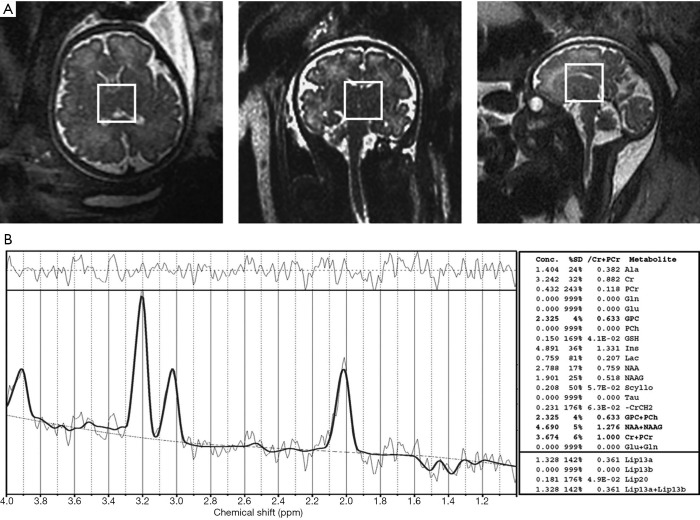
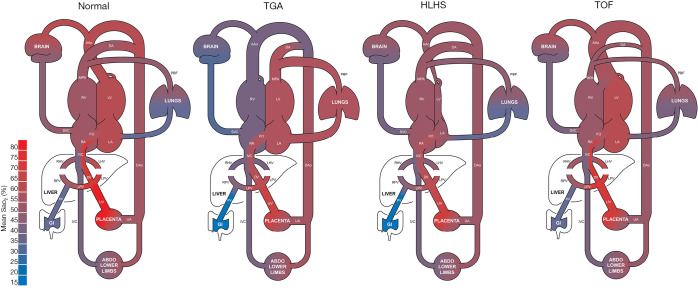
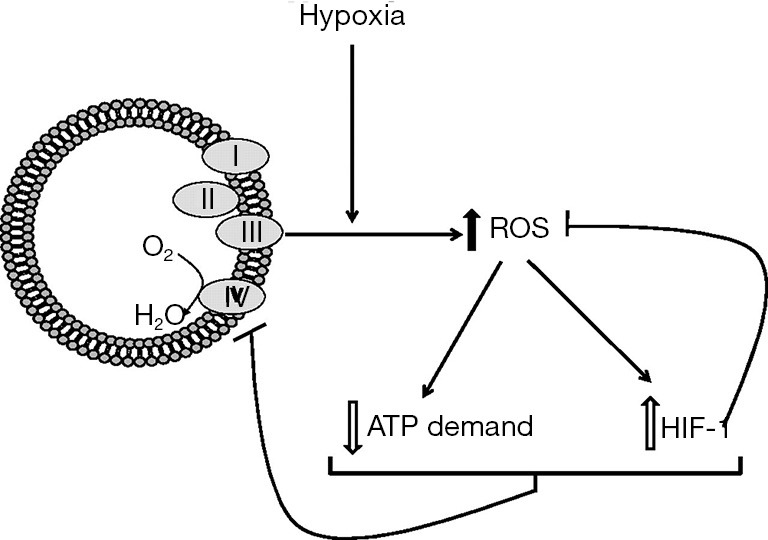
Following the improvements in the clinical management of patients with congenital heart disease (CHD) and their increased survival, neurodevelopmental outcome has become an emerging priority in pediatric cardiology. Large-scale efforts have been made to protect the brain during the postnatal, surgical, and postoperative period; however, the presence of brain immaturity and injury at birth suggests in utero and peripartum disturbances. Over the past decade, there has been considerable interest and investigations on fetal brain growth in the setting of CHD. Advancements in fetal brain imaging have identified abnormal brain development in fetuses with CHD from the macrostructural (brain volumes and cortical folding) down to the microstructural (biochemistry and water diffusivity) scale, with more severe forms of CHD showing worse disturbances and brain abnormalities starting as early as the first trimester. Anomalies in common genetic developmental pathways and diminished cerebral substrate delivery secondary to altered cardiovascular physiology are the forefront hypotheses, but other factors such as impaired placental function and maternal psychological stress have surfaced as important contributors to fetal brain immaturity in CHD. The characterization and timing of fetal brain disturbances and their associated mechanisms are important steps for determining preventative prenatal interventions, which may provide a stronger foundation for the developing brain during childhood.
Keywords: Fetal; brain; congenital heart disease (CHD); imaging.
2021 Translational Pediatrics. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tp-20-224). The series “Pre-natal Diagnosis in Congenital Heart Defects” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous