

Point-of-care microchip electrophoresis for integrated anemia and hemoglobin variant testing
- PMID: 34585199
- PMCID: PMC9714341
- DOI: 10.1039/d1lc00371b
Point-of-care microchip electrophoresis for integrated anemia and hemoglobin variant testing
Abstract
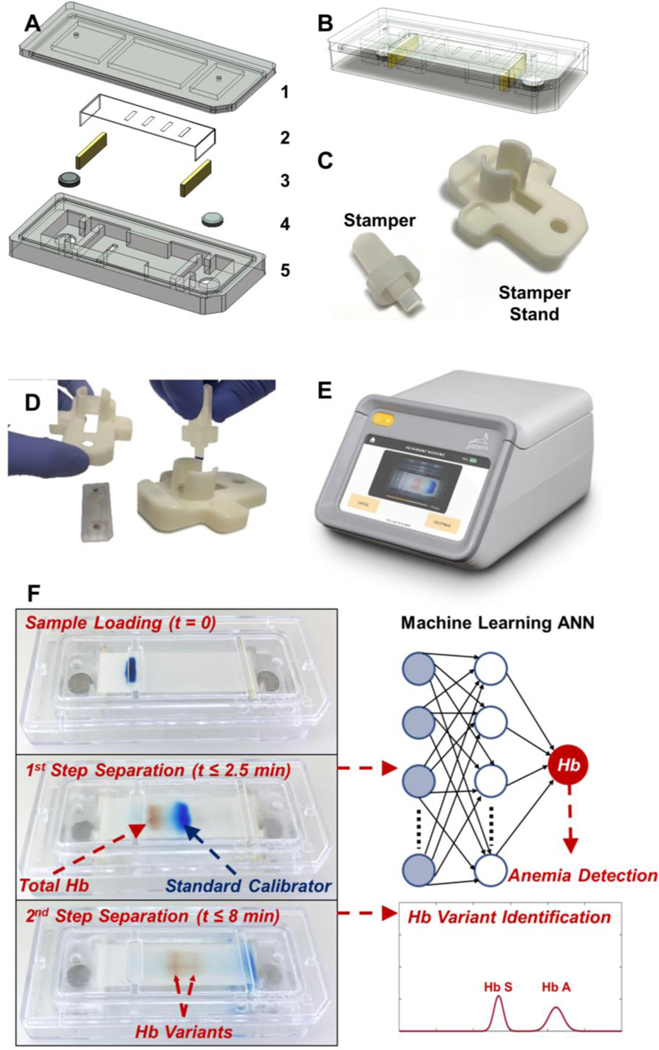
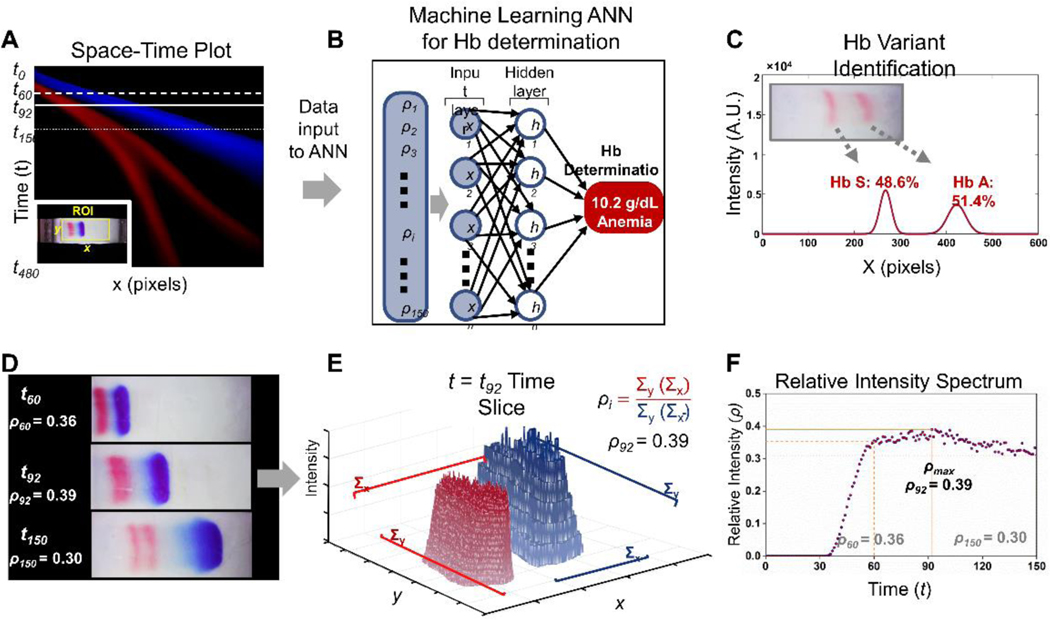
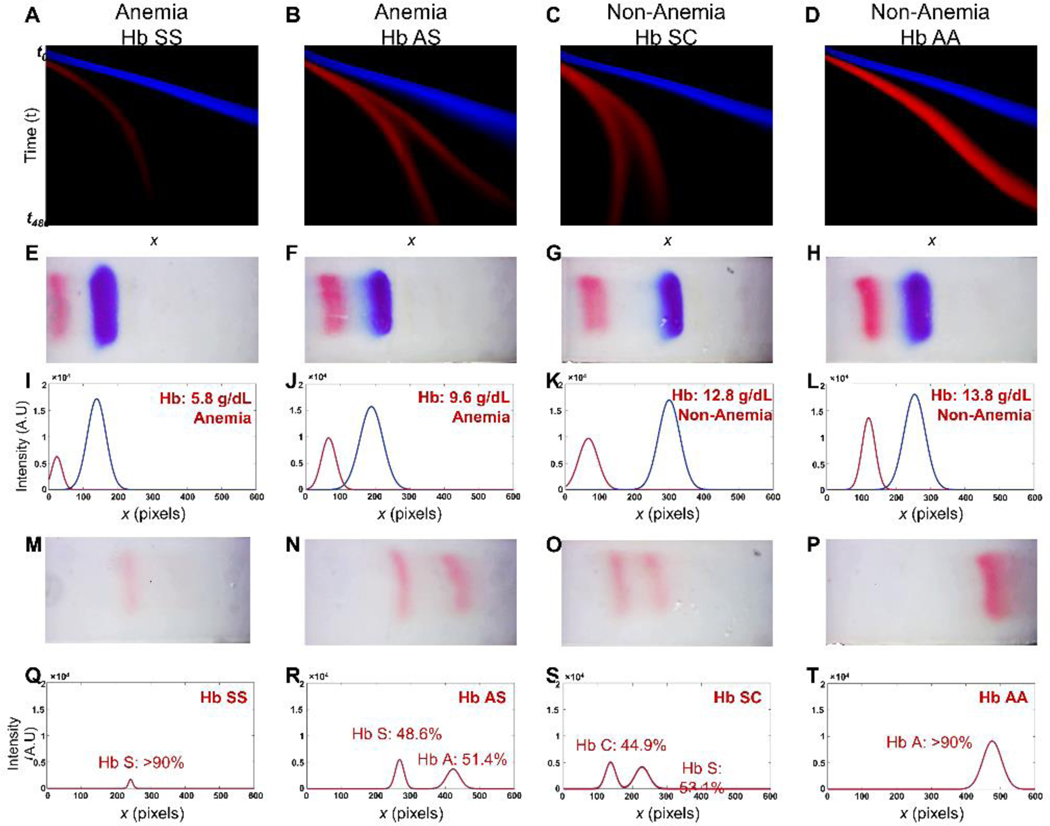
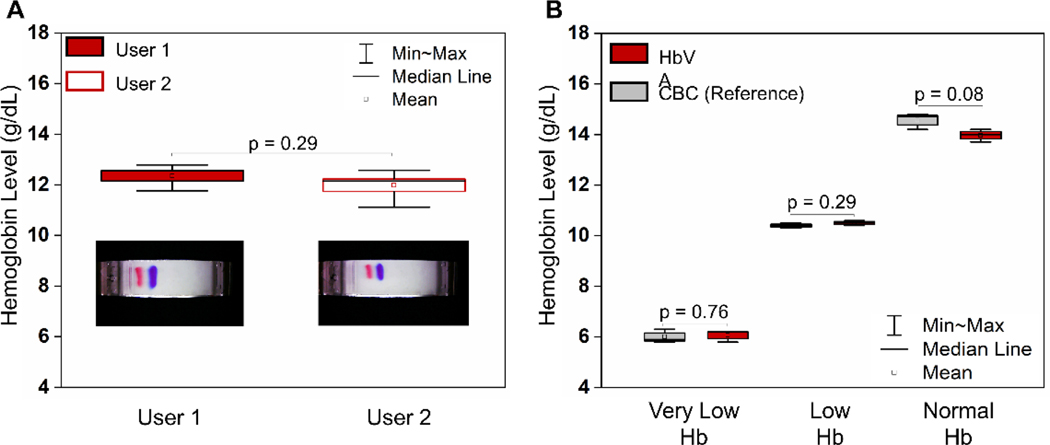
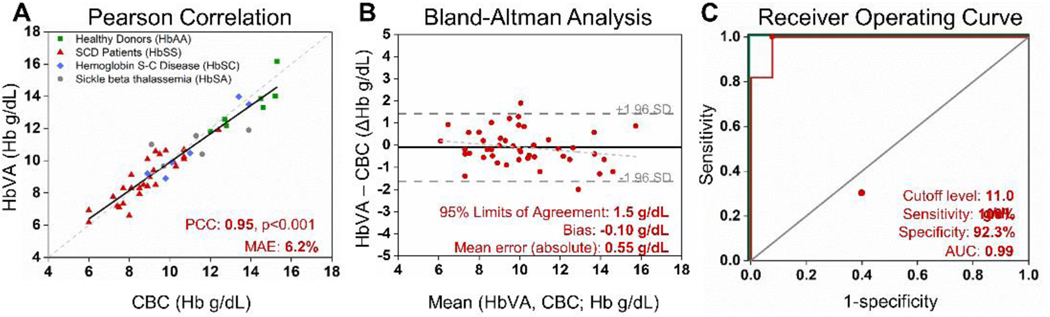
Anemia affects over 25% of the world's population with the heaviest burden borne by women and children. Genetic hemoglobin (Hb) variants, such as sickle cell disease, are among the major causes of anemia. Anemia and Hb variant are pathologically interrelated and have an overlapping geographical distribution. We present the first point-of-care (POC) platform to perform both anemia detection and Hb variant identification, using a single paper-based electrophoresis test. Feasibility of this new integrated diagnostic approach is demonstrated via testing individuals with anemia and/or sickle cell disease. Hemoglobin level determination is performed by an artificial neural network (ANN) based machine learning algorithm, which achieves a mean absolute error of 0.55 g dL-1 and a bias of -0.10 g dL-1 against the gold standard (95% limits of agreement: 1.5 g dL-1) from Bland-Altman analysis on the test set. Resultant anemia detection is achieved with 100% sensitivity and 92.3% specificity. With the same tests, subjects with sickle cell disease were identified with 100% sensitivity and specificity. Overall, the presented platform enabled, for the first time, integrated anemia detection and hemoglobin variant identification using a single point-of-care test.
Conflict of interest statement
Competing interests of Case Western Reserve University employees are overseen and managed by the Conflict of Interests Committee according to a Conflict-of-Interest Management Plan.
Figures
References
-
- T. W. H. Organization.
-
- W. H. Organization, WHO Global Database on Anaemia, 2008.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical