

Coronary Artery Calcification and Plaque Characteristics in People Living With HIV: A Systematic Review and Meta-Analysis
- PMID: 34585590
- PMCID: PMC8649136
- DOI: 10.1161/JAHA.120.019291
Coronary Artery Calcification and Plaque Characteristics in People Living With HIV: A Systematic Review and Meta-Analysis
Abstract
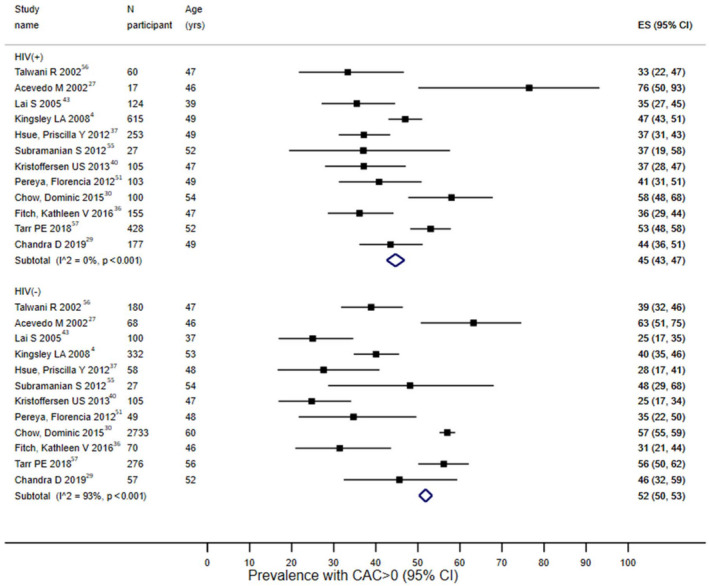
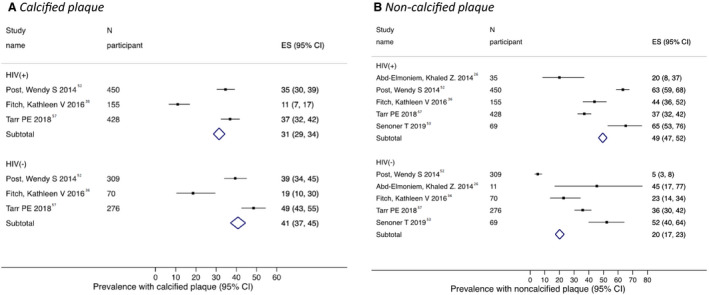
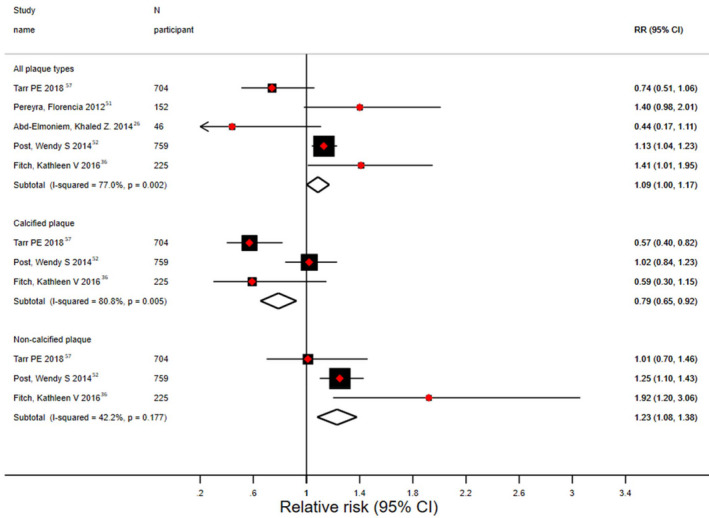
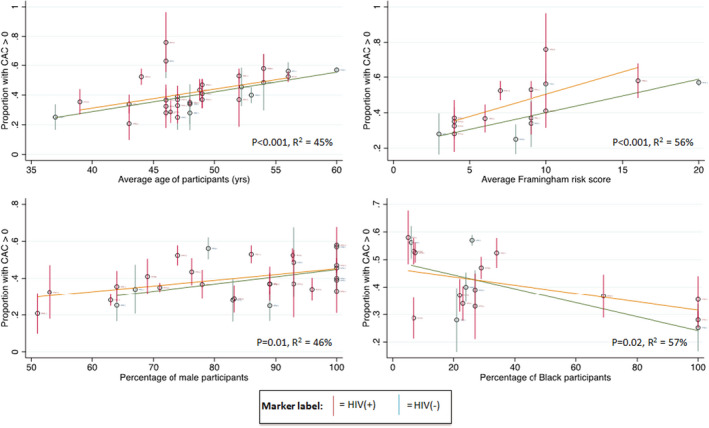
Background Studies have reported that people living with HIV have higher burden of subclinical cardiovascular disease, but the data are not adequately synthesized. We performed meta-analyses of studies of coronary artery calcium and coronary plaque in people living with HIV. Methods and Results We performed systematic search in electronic databases, and data were abstracted in standardized forms. Study-specific estimates were pooled using meta-analysis. 43 reports representing 27 unique studies and involving 10 867 participants (6699 HIV positive, 4168 HIV negative, mean age 52 years, 86% men, 32% Black) were included. The HIV-positive participants were younger (mean age 49 versus 57 years) and had lower Framingham Risk Score (mean score 6 versus 18) compared with the HIV-negative participants. The pooled estimate of percentage with coronary artery calcium >0 was 45% (95% CI, 43%-47%) for HIV-positive participants, and 52% (50%-53%) for HIV-negative participants. This difference was no longer significant after adjusting for difference in Framingham Risk Score between the 2 groups. The odds ratio of coronary artery calcium progression for HIV-positive versus -negative participants was 1.64 (95% CI, 0.91-2.37). The pooled estimate for prevalence of noncalcified plaque was 49% (95% CI, 47%-52%) versus 20% (95% CI, 17%-23%) for HIV-positive versus HIV-negative participants, respectively. Odds ratio for noncalcified plaque for HIV-positive versus -negative participants was 1.23 (95% CI, 1.08-1.38). There was significant heterogeneity that was only partially explained by available study-level characteristics. Conclusions People living with HIV have higher prevalence of noncalcified coronary plaques and similar prevalence of coronary artery calcium, compared with HIV-negative individuals. Future studies on coronary artery calcium and plaque progression can further elucidate subclinical atherosclerosis in people living with HIV.
Keywords: calcium score; cardiovascular disease; coronary artery calcium; coronary plaque; human immunodeficiency virus; subclinical atherosclerosis.
Conflict of interest statement
None.
Figures

References
-
- Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, Lauer MS, Post WS, Raggi P, Redberg RF, et al. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2007;49:378–402. DOI: 10.1016/j.jacc.2006.10.001. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
