

Associations of Maternal Serum Perfluoroalkyl Substances Concentrations with Early Adolescent Bone Mineral Content and Density: The Health Outcomes and Measures of the Environment (HOME) Study
- PMID: 34585601
- PMCID: PMC8480151
- DOI: 10.1289/EHP9424
Associations of Maternal Serum Perfluoroalkyl Substances Concentrations with Early Adolescent Bone Mineral Content and Density: The Health Outcomes and Measures of the Environment (HOME) Study
Abstract
Background: Per- and polyfluoroalkyl substances (PFAS) may impair bone accrual and strength via endocrine disruption and nuclear receptor agonism, but human studies are primarily of adults or cross-sectional.
Objectives: We assessed associations of individual PFAS and their mixture during pregnancy with child bone mineral content (BMC) and areal bone mineral density (aBMD) at age 12 y.
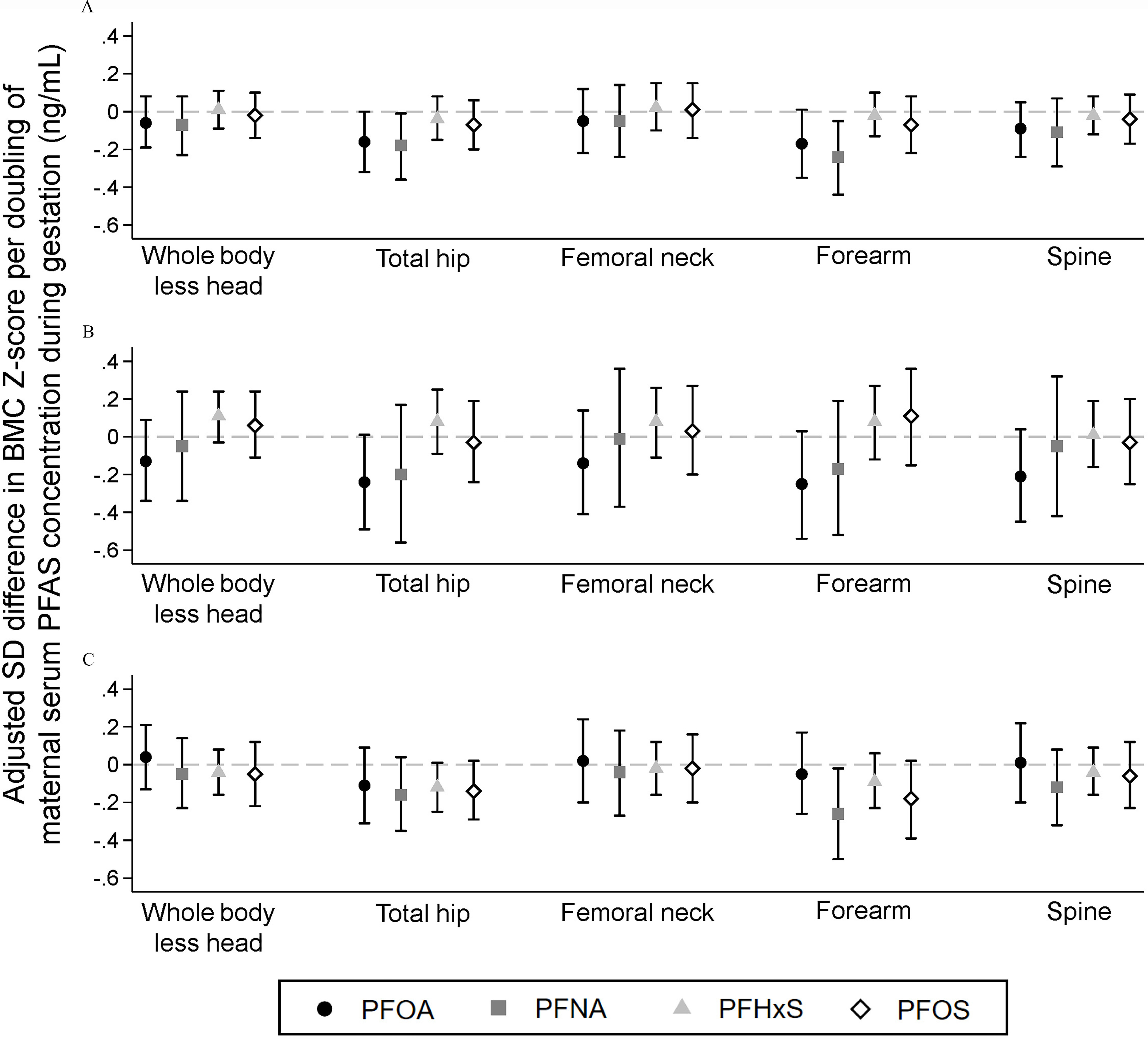
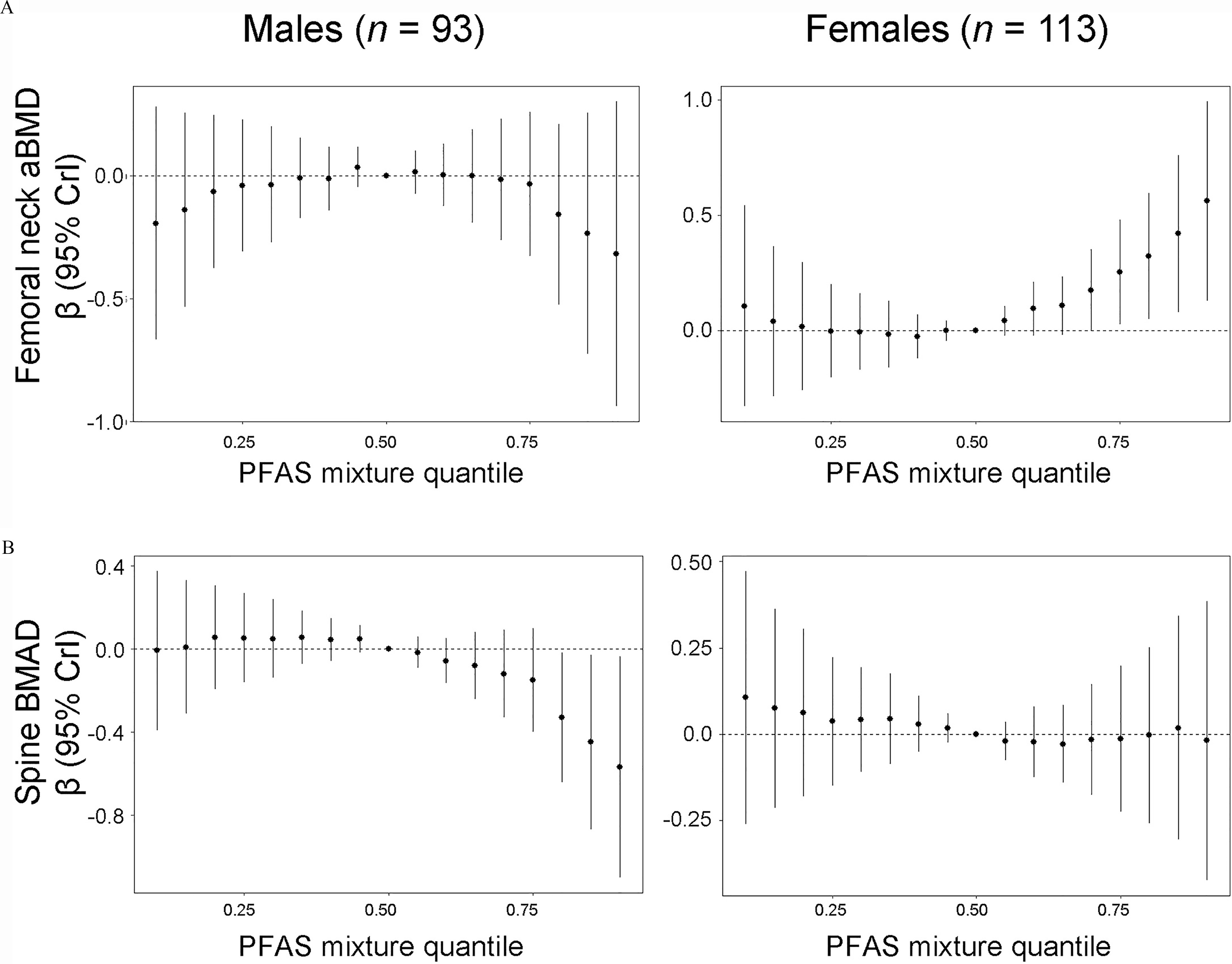
Methods: Among 206 mother-child pairs enrolled in a prospective cohort (2003-2006), we quantified perfluorooctanoic acid (PFOA), perfluorononanoic acid (PFNA), perfluorohexane sulfonic acid (PFHxS), and perfluorooctane sulfonic acid (PFOS) in maternal serum collected during gestation or delivery. When children were age 12 y, we performed dual energy X-ray absorptiometry and calculated BMC, aBMD, and bone mineral apparent density (BMAD) -scores for six skeletal sites. We estimated covariate-adjusted -score differences per doubling of individual PFAS using linear regression and assessed the PFAS mixture using quantile g-computation and Bayesian kernel machine regression. We explored whether associations were modified by child's sex or mediated by whole-body lean mass.
Results: In covariate-adjusted models, we found that higher maternal serum concentrations of PFOA, PFNA, and the PFAS mixture were associated with lower total hip and forearm (one-third distal radius) BMC -scores in children. Differences in forearm BMC -scores were [95% confidence interval (CI): , 0.01] and (95% CI: , ) per doubling of PFOA and PFNA, respectively, and (95% CI: , ) per quartile increase in the PFAS mixture. Child's sex modified PFOA associations for some skeletal sites; for example, differences in spine BMAD -score per doubling were (95% CI: , ) among males and 0.07 (95% CI: , 0.30) among females (modification ). Except for PFNA among females, these associations were not mediated by whole-body lean mass.
Discussion: Maternal PFAS concentrations during pregnancy may be associated with lower bone mineral accrual and strength in early adolescence. https://doi.org/10.1289/EHP9424.
Figures
Comment in
-
A Measure of Strength: Developmental PFAS Exposures and Bone Mineral Content in Adolescence.Environ Health Perspect. 2021 Dec;129(12):124002. doi: 10.1289/EHP10551. Epub 2021 Dec 17. Environ Health Perspect. 2021. PMID: 34918944 Free PMC article.
References
-
- Bailey DA, McKay HA, Mirwald RL, Crocker PR, Faulkner RA. 1999. A six-year longitudinal study of the relationship of physical activity to bone mineral accrual in growing children: the University of Saskatchewan bone mineral accrual study. J Bone Miner Res 14(10):1672–1679, PMID: 10491214, 10.1359/jbmr.1999.14.10.1672. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources