

Comparison of Long-term Clinical Outcomes of Skeletonized vs Pedicled Internal Thoracic Artery Harvesting Techniques in the Arterial Revascularization Trial
- PMID: 34586338
- PMCID: PMC8482293
- DOI: 10.1001/jamacardio.2021.3866
Comparison of Long-term Clinical Outcomes of Skeletonized vs Pedicled Internal Thoracic Artery Harvesting Techniques in the Arterial Revascularization Trial
Abstract
Importance: Recent evidence has suggested that skeletonization of the internal thoracic artery (ITA) is associated with worse clinical outcomes in patients undergoing coronary artery bypass surgery (CABG).
Objective: To compare the long-term clinical outcomes of skeletonized and pedicled ITA for CABG.
Design, setting, and participants: The Arterial Revascularization Trial (ART) was a 2-group, multicenter trial comparing the use of a bilateral ITA vs a single ITA for CABG at 10 years. Patients in the ART trial were stratified by ITA harvesting technique: skeletonized vs pedicled. Data were collected from June 2004 to December 2017, and data were analyzed from June to July 2021.
Interventions: In this analysis, the 10-year clinical outcomes were compared between patients who received skeletonized vs pedicled ITAs.
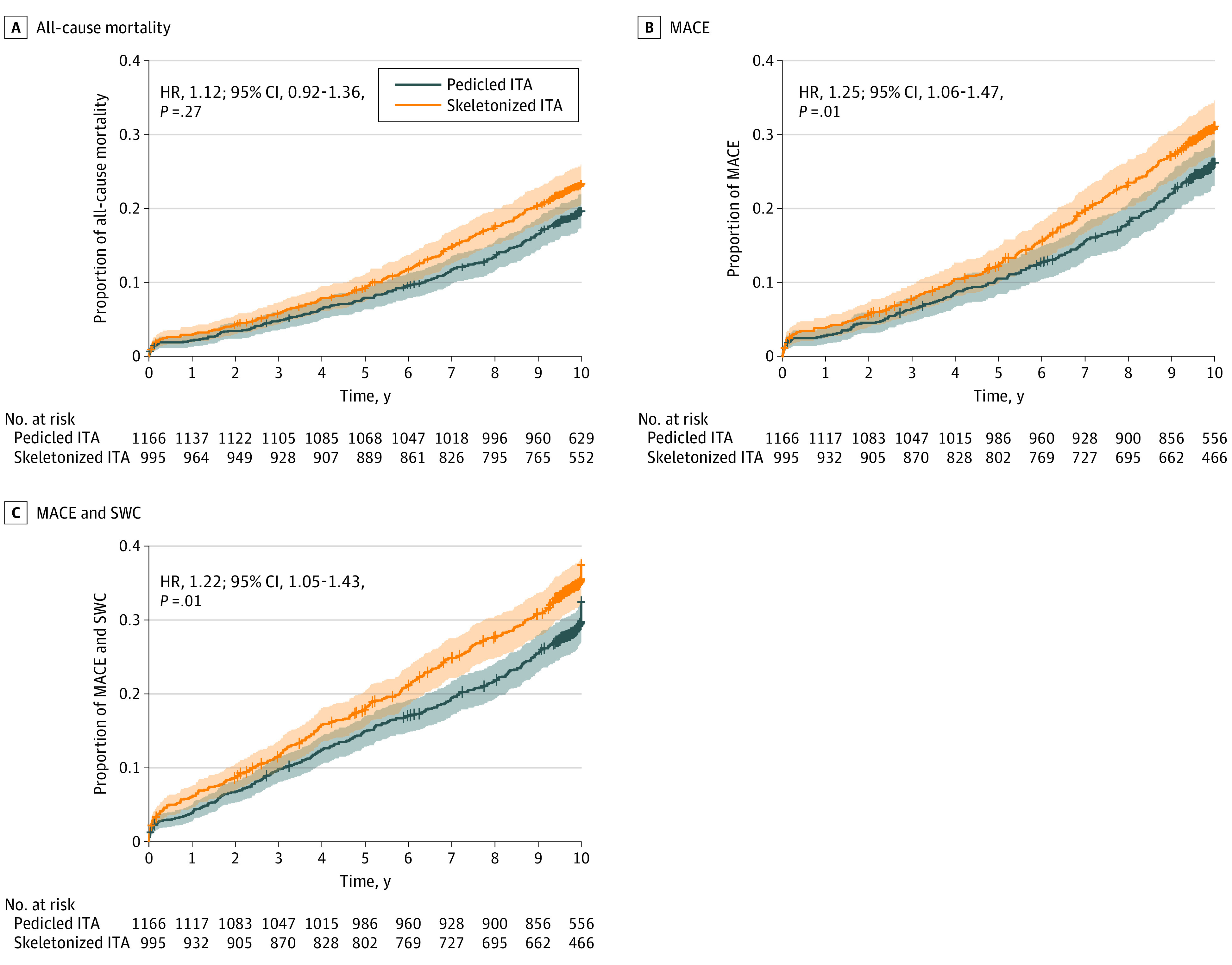
Main outcomes and measures: The primary outcome was all-cause mortality. The secondary outcomes were a composite of major adverse cardiac events (MACE) including all-cause mortality, myocardial infarction, and repeated revascularization and a composite including MACE and sternal wound complication (SWC). Cox regression and propensity score matching were used.
Results: Of 2161 included patients, 295 (13.7%) were female, and the median (interquartile range) age was 65.0 (58.0-70.0) years. At 10 years, the risk of all-cause mortality was not significantly different between the pedicled and skeletonized groups (hazard ratio [HR], 1.12; 95% CI, 0.92-1.36; P = .27). However, the long-term risks of the secondary outcomes were significantly higher in the skeletonized group compared with the pedicled group (MACE: HR, 1.25; 95% CI, 1.06-1.47; P = .01; MACE and SWC: HR, 1.22; 95% CI, 1.05-1.43; P = .01). The difference was not seen when considering only patients operated on by surgeons who enrolled 51 patients or more in the trial (MACE: HR, 1.07; 95% CI, 0.82-1.39; P = .62; MACE and SWC: HR, 1.04; 95% CI, 0.80-1.34; P = .78).
Conclusions and relevance: While the long-term survival of patients was not different between groups, the rate of adverse cardiovascular events was consistently higher in the skeletonized group and the difference was associated with surgeon-related factors. Further evidence on the outcome of skeletonized ITA is needed.
Conflict of interest statement
Figures
Comment in
-
Coronary Artery Bypass Grafting With the Internal Thoracic Artery: A Great Operation With Some Unanswered Questions.JAMA Cardiol. 2021 Dec 1;6(12):1362-1363. doi: 10.1001/jamacardio.2021.3863. JAMA Cardiol. 2021. PMID: 34586360 No abstract available.
References
-
- Hillis LD, Smith PK, Anderson JL, et al. . 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(23):e652-e735. - PubMed
-
- Gaudino M, Bakaeen FG, Benedetto U, et al. ; ATLANTIC (Arterial Grafting International Consortium) Alliance Members . Arterial grafts for coronary bypass: a critical review after the publication of ART and RADIAL. Circulation. 2019;140(15):1273-1284. doi:10.1161/CIRCULATIONAHA.119.041096 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
