

Prevalence of Dyslipidemia and Availability of Lipid-Lowering Medications Among Primary Health Care Settings in China
- PMID: 34586366
- PMCID: PMC8482054
- DOI: 10.1001/jamanetworkopen.2021.27573
Prevalence of Dyslipidemia and Availability of Lipid-Lowering Medications Among Primary Health Care Settings in China
Abstract
Importance: Dyslipidemia, the prevalence of which historically has been low in China, is emerging as the second leading yet often unaddressed factor associated with the risk of cardiovascular diseases. However, recent national data on the prevalence, treatment, and control of dyslipidemia are lacking.
Objective: To assess the prevalence, treatment, and control of dyslipidemia in community residents and the availability of lipid-lowering medications in primary care institutions in China.
Design, setting, and participants: This cross-sectional study used data from the China-PEACE (Patient-Centered Evaluative Assessment of Cardiac Events) Million Persons Project, which enrolled 2 660 666 community residents aged 35 to 75 years from all 31 provinces in China between December 2014 and May 2019, and the China-PEACE primary health care survey of 3041 primary care institutions. Data analysis was performed from June 2019 to March 2021.
Exposures: Study period.
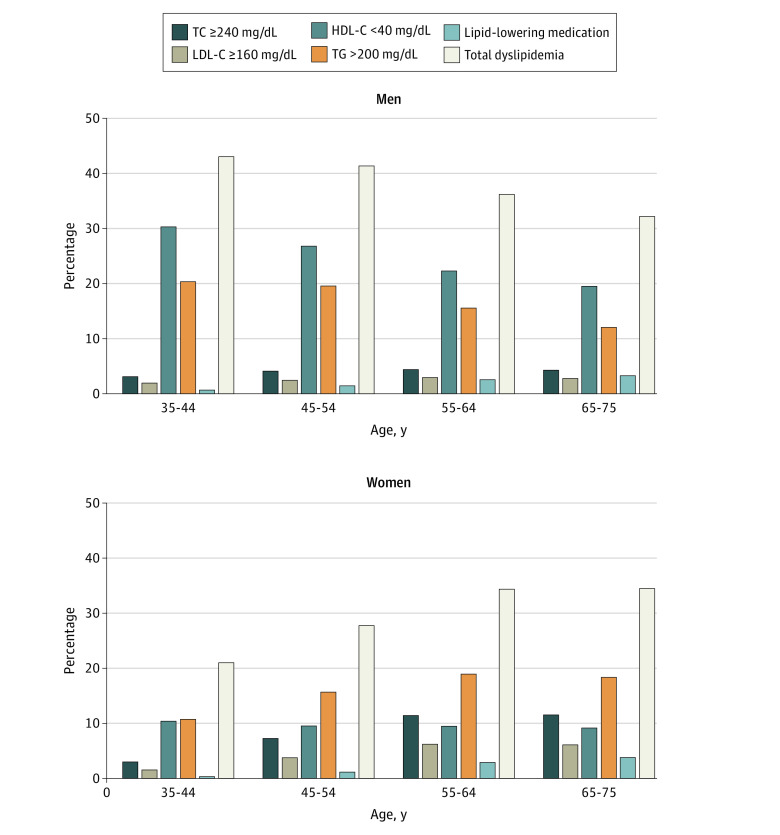
Main outcomes and measures: The main outcome was the prevalence of dyslipidemia, which was defined as total cholesterol greater than or equal to 240 mg/dL, low-density lipoprotein cholesterol (LDL-C) greater than or equal to 160 mg/dL, high-density lipoprotein cholesterol (HDL-C) less than 40 mg/dL, triglycerides greater than or equal to 200 mg/dL, or self-reported use of lipid-lowering medications, in accordance with the 2016 Chinese Adult Dyslipidemia Prevention Guideline.
Results: This study included 2 314 538 participants with lipid measurements (1 389 322 women [60.0%]; mean [SD] age, 55.8 [9.8] years). Among them, 781 865 participants (33.8%) had dyslipidemia. Of 71 785 participants (3.2%) who had established atherosclerotic cardiovascular disease (ASCVD) and were recommended by guidelines for lipid-lowering medications regardless of LDL-C levels, 10 120 (14.1%) were treated. The overall control rate of LDL-C (≤70 mg/dL) among adults with established ASCVD was 26.6% (19 087 participants), with the control rate being 44.8% (4535 participants) among those who were treated and 23.6% (14 552 participants) among those not treated. Of 236 579 participants (10.2%) with high risk of ASCVD, 101 474 (42.9%) achieved LDL-C less than or equal to 100 mg/dL. Among participants with established ASCVD, advanced age (age 65-75 years, odds ratio [OR], 0.63; 95% CI, 0.56-0.70), female sex (OR, 0.56; 95% CI, 0.53-0.58), lower income (reference category), smoking (OR, 0.89; 95% CI, 0.85-0.94), alcohol consumption (OR, 0.87; 95% CI, 0.83-0.92), and not having diabetes (reference category) were associated with lower control of LDL-C. Among participants with high risk of ASCVD, younger age (reference category) and female sex (OR, 0.58; 95% CI, 0.56-0.59) were associated with lower control of LDL-C. Of 3041 primary care institutions surveyed, 1512 (49.7%) stocked statin and 584 (19.2%) stocked nonstatin lipid-lowering drugs. Village clinics in rural areas had the lowest statin availability.
Conclusions and relevance: These findings suggest that dyslipidemia has become a major public health problem in China and is often inadequately treated and uncontrolled. Statins were available in less than one-half of the primary care institutions. Strategies aimed at detection, prevention, and treatment are needed.
Conflict of interest statement
Figures

References
-
- Report on Cardiovascular Disease in China 2015. National Center for Cardiovascular Disease; 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
