

TRI-SCORE: a new risk score for in-hospital mortality prediction after isolated tricuspid valve surgery
- PMID: 34586392
- PMCID: PMC8843795
- DOI: 10.1093/eurheartj/ehab679
TRI-SCORE: a new risk score for in-hospital mortality prediction after isolated tricuspid valve surgery
Abstract
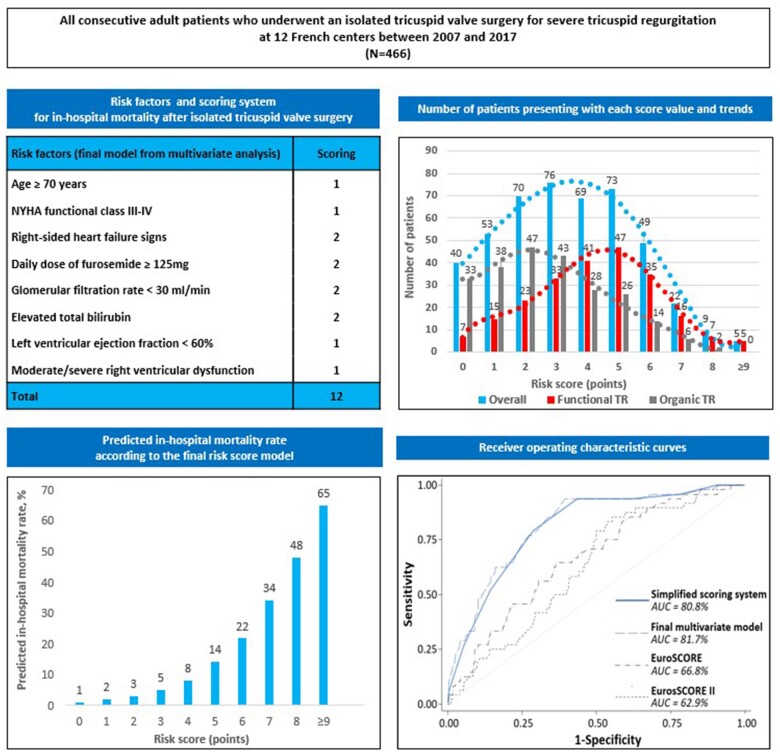
Aims: Isolated tricuspid valve surgery (ITVS) is considered to be a high-risk procedure, but in-hospital mortality is markedly variable. This study sought to develop a dedicated risk score model to predict the outcome of patients after ITVS for severe tricuspid regurgitation (TR).
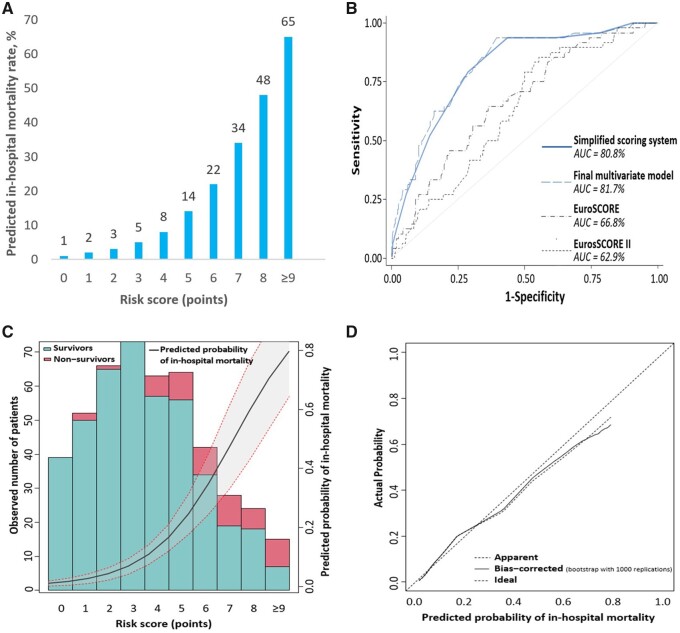
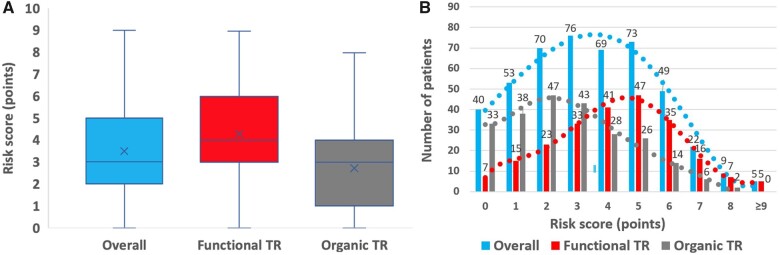
Methods and results: All consecutive adult patients who underwent ITVS for severe non-congenital TR at 12 French centres between 2007 and 2017 were included. We identified 466 patients (60 ± 16 years, 49% female, functional TR in 49%). In-hospital mortality rate was 10%. We derived and internally validated a scoring system to predict in-hospital mortality using multivariable logistic regression and bootstrapping with 1000 re-samples. The final risk score ranged from 0 to 12 points and included eight parameters: age ≥70 years, New York Heart Association Class III-IV, right-sided heart failure signs, daily dose of furosemide ≥125 mg, glomerular filtration rate <30 mL/min, elevated bilirubin, left ventricular ejection fraction <60%, and moderate/severe right ventricular dysfunction. Tricuspid regurgitation mechanism was not an independent predictor of outcome. Observed and predicted in-hospital mortality rates increased from 0% to 60% and from 1% to 65%, respectively, as the score increased from 0 up to ≥9 points. Apparent and bias-corrected areas under the receiver operating characteristic curves were 0.81 and 0.75, respectively, much higher than the logistic EuroSCORE (0.67) or EuroSCORE II (0.63).
Conclusion: We propose TRI-SCORE as a dedicated risk score model based on eight easy to ascertain parameters to inform patients and physicians regarding the risk of ITVS and guide the clinical decision-making process of patients with severe TR, especially as transcatheter therapies are emerging (www.tri-score.com).
Keywords: Outcome; Surgery; Tricuspid regurgitation; Risk score.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
A new tool for the forgotten valve: a score to predict the risk of surgery.Eur Heart J. 2022 Feb 12;43(7):663-665. doi: 10.1093/eurheartj/ehab799. Eur Heart J. 2022. PMID: 34849713 No abstract available.
References
-
- Topilsky Y, Maltais S, Medina Inojosa J, Oguz D, Michelena H, Maalouf J, Mahoney DW, Enriquez-Sarano M. Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc Imaging 2019;12:433–442. - PubMed
-
- Wang N, Fulcher J, Abeysuriya N, McGrady M, Wilcox I, Celermajer D, Lal S. Tricuspid regurgitation is associated with increased mortality independent of pulmonary pressures and right heart failure: a systematic review and meta-analysis. Eur Heart J 2019;40:476–484. - PubMed
-
- Messika-Zeitoun D, Verta P, Gregson J, Pocock SJ, Boero I, Feldman TE, Abraham WT, Lindenfeld J, Bax J, Leon M, Enriquez-Sarano M. Impact of tricuspid regurgitation on survival in patients with heart failure: a large electronic health record patient-level database analysis. Eur J Heart Fail 2020;22:1803–1813. - PubMed
-
- Dreyfus J, Flagiello M, Bazire B, Eggenspieler F, Viau F, Riant E, Mbaki Y, Bohbot Y, Eyharts D, Senage T, Dubrulle H, Nicol M, Doguet F, Nguyen V, Coisne A, Le Tourneau T, Lavie-Badie Y, Tribouilloy C, Donal E, Tomasi J, Habib G, Selton-Suty C, Raffoul R, Iung B, Obadia JF, Messika-Zeitoun D. Isolated tricuspid valve surgery: impact of aetiology and clinical presentation on outcomes. Eur Heart J 2020;41:4304–4317. - PubMed
-
- Dreyfus J, Ghalem N, Garbarz E, Cimadevilla C, Nataf P, Vahanian A, Caranhac G, Messika-Zeitoun D. Timing of referral of patients with severe isolated tricuspid valve regurgitation to surgeons (from a French Nationwide Database). Am J Cardiol 2018;122:323–326. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
