

Efficacy and safety of nivolumab in Japanese patients with first recurrence of glioblastoma: an open-label, non-comparative study
- PMID: 34586548
- PMCID: PMC8580927
- DOI: 10.1007/s10147-021-02028-1
Efficacy and safety of nivolumab in Japanese patients with first recurrence of glioblastoma: an open-label, non-comparative study
Abstract
Background: An open-label, non-comparative study assessed the efficacy and safety of nivolumab in Japanese patients with first recurrence glioblastoma.
Methods: Patients with first recurrence of histologically confirmed World Health Organization Grade IV glioma, after treatment with temozolomide and radiotherapy, received nivolumab 3 mg/kg every 2 weeks until confirmed disease progression (Response Assessment in Neuro-Oncology criteria) or toxicity. Primary endpoint was 1-year overall survival rate assessed by Bayesian approach. The prespecified efficacy criterion was that the Bayesian posterior probability threshold for exceeding the 1-year overall survival of bevacizumab (34.5%) from the Japanese phase 2 study (JO22506) would be 93%.
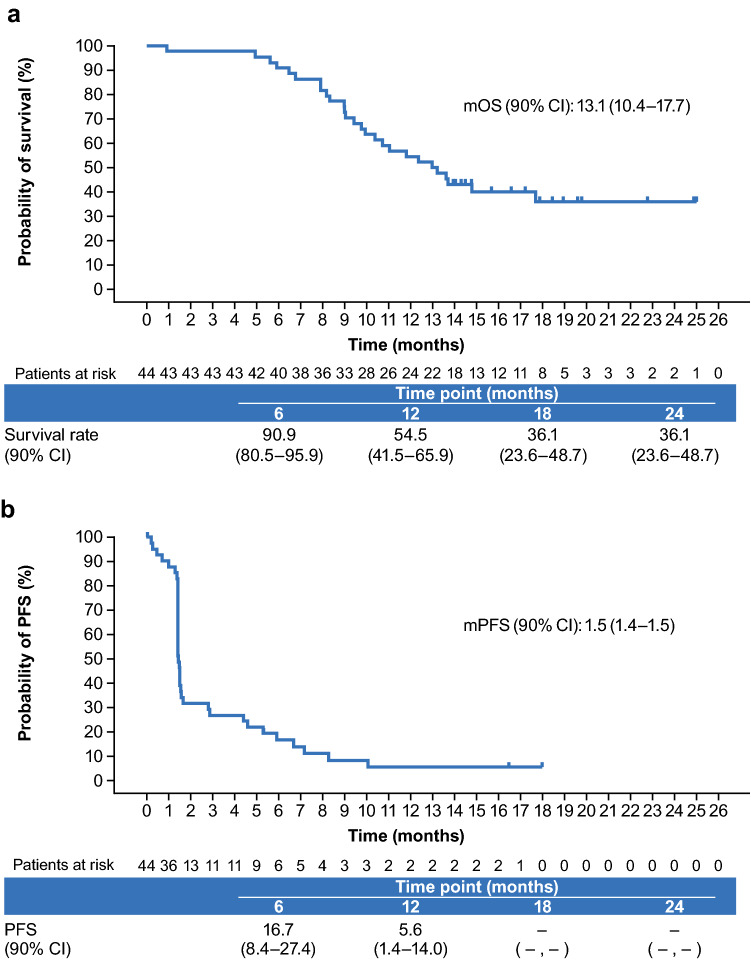
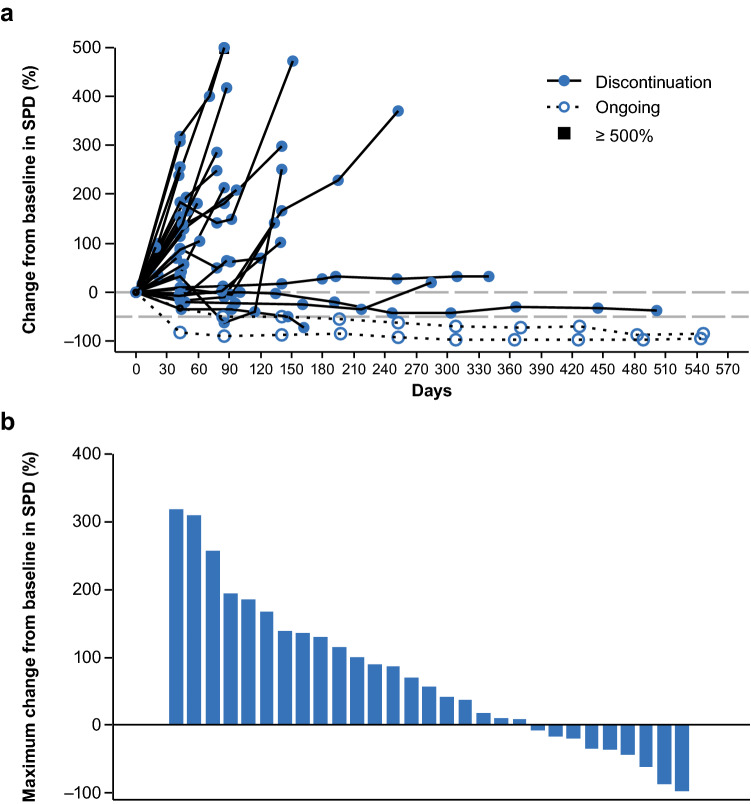
Results: Of the 50 enrolled patients, 44 (88.0%) had recurrent malignant glioma (glioblastoma, gliosarcoma), and of these, 26 (59.1%) had at least one measurable lesion at baseline. The Bayesian posterior mean 1-year overall survival (90% Bayesian credible intervals) with nivolumab was 54.4% (42.27-66.21), and the Bayesian posterior probability of exceeding the threshold of the 1-year overall survival rate of bevacizumab (34.5%) was 99.7%. Median (90% confidence interval) overall and progression-free survival was 13.1 (10.4-17.7) and 1.5 (1.4-1.5) months, respectively. One partial response was observed (objective response rate 1/26 evaluable patients [3.8%]). Treatment-related adverse event rates were 14.0% for Grade 3-4 and 2.0% for Grade 5; most adverse events resolved and were manageable.
Conclusions: The 1-year overall survival with nivolumab monotherapy in Japanese patients with glioblastoma met the prespecified efficacy criterion. The safety profile of nivolumab was consistent with that observed in other tumor types.
Clinical trial registration: JapicCTI-152967.
Keywords: Bayesian approach; Bevacizumab; Clinical Trial; Glioblastoma; Nivolumab; Phase II; Programmed cell death.
© 2021. The Author(s).
Conflict of interest statement
T. Aoki, N. Kagawa, T. Wakabayashi, S. Yamaguchi, E. Ishikawa, S. Suehiro, J. Kuroda, Y. Iwadate, M. Natsumeda, Y. Nakazato, and S. Hagihara have no conflicts of interest to declare. K. Sugiyama has received research funding from Ono Pharmaceutical Co., Ltd., Daiichi-Sankyo Co., Ltd., and Sumitomo Dainippon Pharma Co. Ltd. Y. Arakawa has received research funding from Ono Pharmaceutical Co., Ltd., Siemens, Philips, Chugai Pharmaceutical Co., Ltd., Daiichi-Sankyo Co., Ltd., and Taiho Pharmaceutical Co., Ltd.; and honoraria from Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., and Daiichi-Sankyo Co., Ltd. S. Tanaka has received research funding from Eisai Co., Ltd., Ono Pharmaceutical Co., Ltd., and Sumitomo Dainippon Pharma Co. Ltd. Y. Muragaki has received lecture fees, honoraria, or other fees from Eisai Co., Ltd. and Novocure Limited. M. Nagane has received lecture fees, honoraria, or other fees from MSD and Ono Pharmaceutical Co., Ltd.; has received research funding from Toray Industries, Inc., AbbVie Inc., and Ono Pharmaceutical Co., Ltd.; and has received scholarship (incentive) endowments or research grants from Eisai Co., Ltd., Pfizer, Nippon Kayaku Co., Ltd., and Chugai Pharmaceutical Co., Ltd. M. Nakada has received research funding from Ono Pharmaceutical Co., Ltd.; and has received scholarship (incentive) endowments or research grants from Otsuka Pharmaceutical Co., Ltd., Stryker Corporation, Eisai Co., Ltd., MSD, and Chugai Pharmaceutical Co., Ltd. N. Hata has received research funding from Daiichi-Sankyo Co., Ltd. Y. Narita has received research funding from Eisai Co., Ltd., Ono Pharmaceutical Co., Ltd., AbbVie Inc., Bayer AG, Sumitomo Dainippon Pharma Co. Ltd., Taiho Pharmaceutical Co., Ltd., and Daiichi-Sankyo Co., Ltd. Y. Sonoda has received scholarship (incentive) endowments or research grants from Eisai Co., Ltd., Otsuka Pharmaceutical Co., Ltd., and Fujifilm. H. Minami has received lecture fees, honoraria, or other fees from Daiichi-Sankyo Co., Ltd. and Ono Pharmaceutical Co., Ltd.; has received research funding from Amgen Astellas BioPharma K.K., Bayer AG, Bristol-Myers Squibb, Daiichi-Sankyo Co., Ltd., Novartis, Pfizer, and Ono Pharmaceutical Co., Ltd.; and has received scholarship (incentive) endowments or research grants from Astellas, Bayer AG, Bristol-Myers Squibb, Chugai Pharmaceutical Co., Ltd., Daiichi-Sankyo Co., Ltd., Kyowa Kirin, Eli Lilly, Ono Pharmaceutical Co., Ltd., Pfizer, Taiho Pharmaceutical Co., Ltd., and Takeda Pharmaceutical Company Limited. Y. Hirata is an employee and shareholder at Ono Pharmaceutical Co., Ltd. R. Nishikawa has received manuscript fees from Eisai Co., Ltd.; has received research funding from AbbVie Inc., Daiichi-Sankyo Co., Ltd., Ono Pharmaceutical Co., Ltd., Toray Industries, Inc., and Medi-Physics, Inc.; and has received scholarship (incentive) endowments or research grants from Chugai Pharmaceutical Co., Ltd. and MSD.
Figures
References
-
- Narita Y. Epidemiology and standard therapy in gliomas. Jpn J Neurosurg. 2012;21(3):184–191. doi: 10.7887/jcns.21.184. - DOI
-
- Narita Y, Shibui S, Committee of Brain Tumor Registry of Japan supported by the Japan Neurosurgical Society Trends and outcomes in the treatment of gliomas based on data during 2001–2004 from the Brain Tumor Registry of Japan. Neurol Med Chir (Tokyo) 2015;55(4):286–295. doi: 10.2176/nmc.ra.2014-0348. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
