

Acute Management of High-Risk and Intermediate-Risk Pulmonary Embolism in Children: A Review
- PMID: 34587483
- PMCID: PMC8941619
- DOI: 10.1016/j.chest.2021.09.019
Acute Management of High-Risk and Intermediate-Risk Pulmonary Embolism in Children: A Review
Abstract
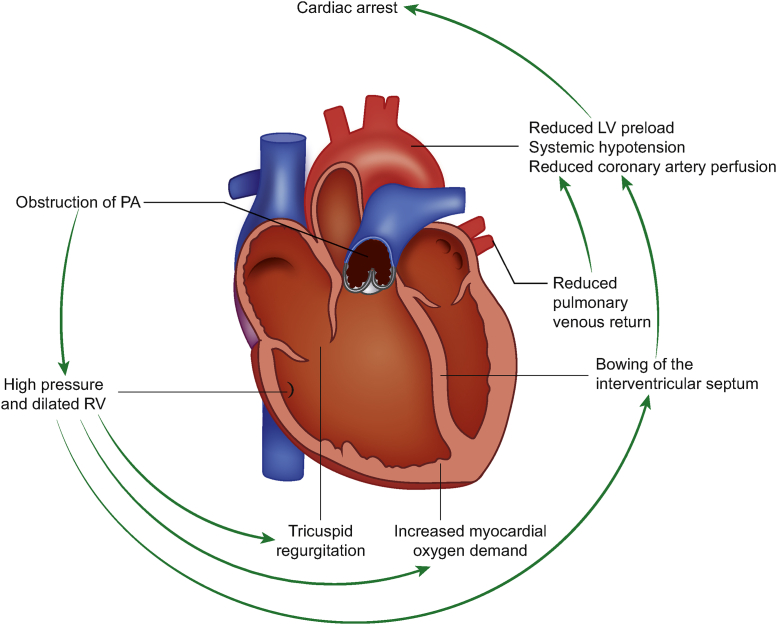
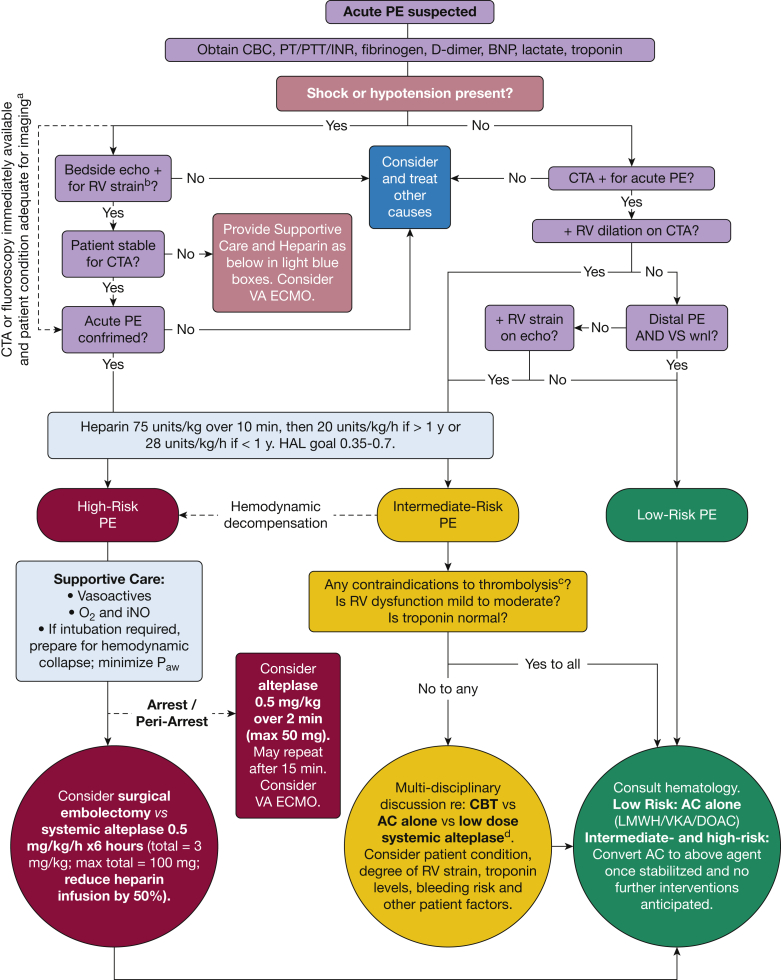
Severe forms of pulmonary embolism (PE) in children, althought rare, cause significant morbidity and mortality. We review the pathophysiologic features of severe (high-risk and intermediate-risk) PE and suggest novel pediatric-specific risk stratifications and an acute treatment algorithm to expedite emergent decision-making. We defined pediatric high-risk PE as causing cardiopulmonary arrest, sustained hypotension, or normotension with signs or symptoms of shock. Rapid primary reperfusion should be pursued with either surgical embolectomy or systemic thrombolysis in conjunction with a heparin infusion and supportive care as appropriate. We defined pediatric intermediate-risk PE as a lack of systemic hypotension or compensated shock, but with evidence of right ventricular strain by imaging, myocardial necrosis by elevated cardiac troponin levels, or both. The decision to pursue primary reperfusion in this group is complex and should be reserved for patients with more severe disease; anticoagulation alone also may be appropriate in these patients. If primary reperfusion is pursued, catheter-based therapies may be beneficial. Acute management of severe PE in children may include systemic thrombolysis, surgical embolectomy, catheter-based therapies, or anticoagulation alone and may depend on patient and institutional factors. Pediatric emergency and intensive care physicians should be familiar with the risks and benefits of each therapy to expedite care. PE response teams also may have added benefit in streamlining care during these critical events.
Keywords: anticoagulation; pediatric pulmonary embolism; surgical embolectomy; thrombolysis.
Copyright © 2021 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Biss T.T., Brandao L.R., Kahr W.H., Chan A.K., Williams S. Clinical features and outcome of pulmonary embolism in children. Br J Haematol. 2008;142(5):808–818. - PubMed
-
- Stein P.D., Kayali F., Olson R.E. Incidence of venous thromboembolism in infants and children: data from the National Hospital Discharge Survey. J Pediatr. 2004;145(4):563–565. - PubMed
-
- Van Ommen C.H., Peters M. Acute pulmonary embolism in childhood. Thromb Res. 2006;118(1):13–25. - PubMed
-
- Andrew M., David M., Adams M., et al. Venous thromboembolic complications (VTE) in children: first analyses of the Canadian Registry of VTE. Blood. 1994;83(5):1251–1257. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
