

Epigenetic Age and the Risk of Incident Atrial Fibrillation
- PMID: 34587750
- PMCID: PMC8671333
- DOI: 10.1161/CIRCULATIONAHA.121.056456
Epigenetic Age and the Risk of Incident Atrial Fibrillation
Abstract
Background: The most prominent risk factor for atrial fibrillation (AF) is chronological age; however, underlying mechanisms are unexplained. Algorithms using epigenetic modifications to the human genome effectively predict chronological age. Chronological and epigenetic predicted ages may diverge in a phenomenon referred to as epigenetic age acceleration (EAA), which may reflect accelerated biological aging. We sought to evaluate for associations between epigenetic age measures and incident AF.
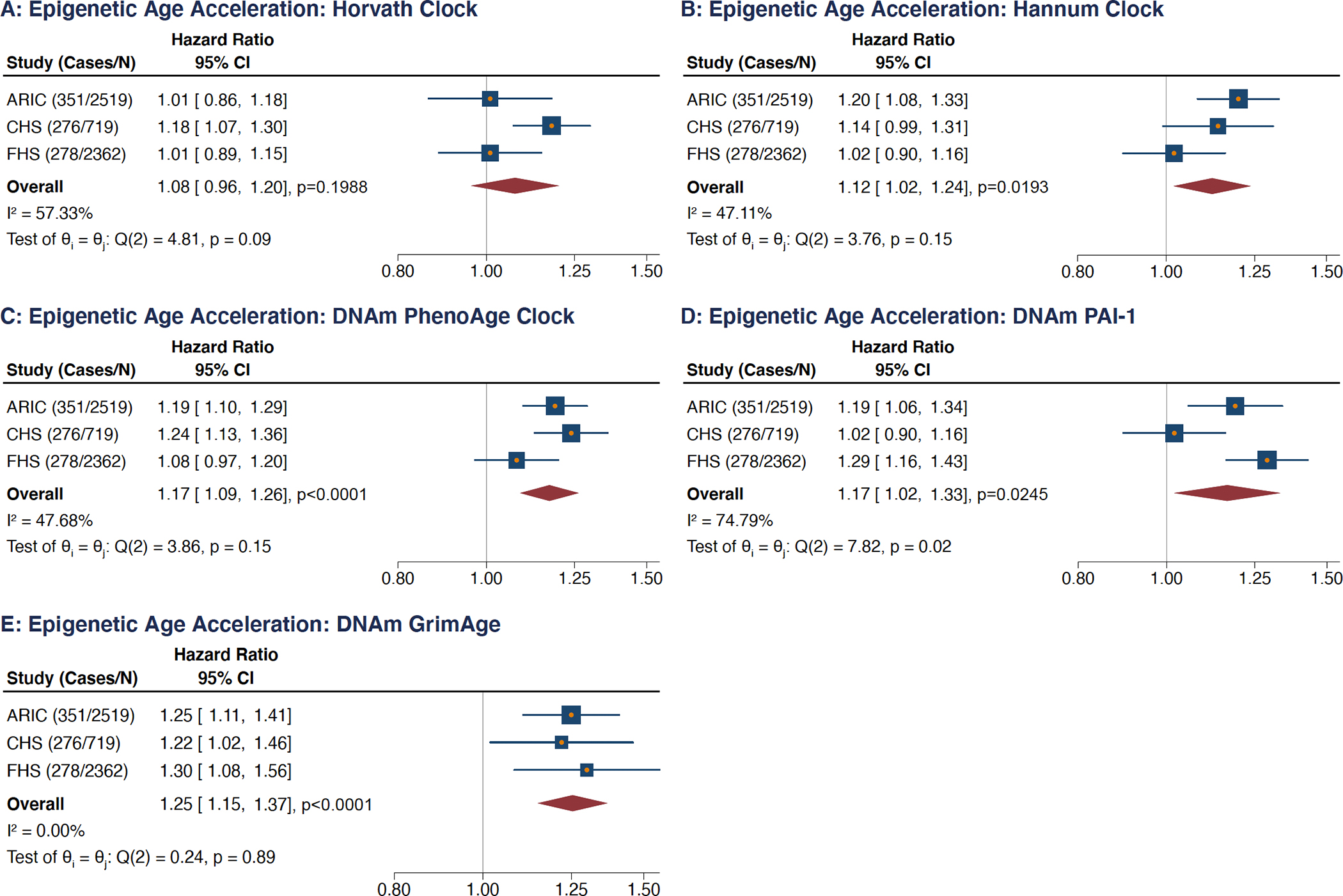
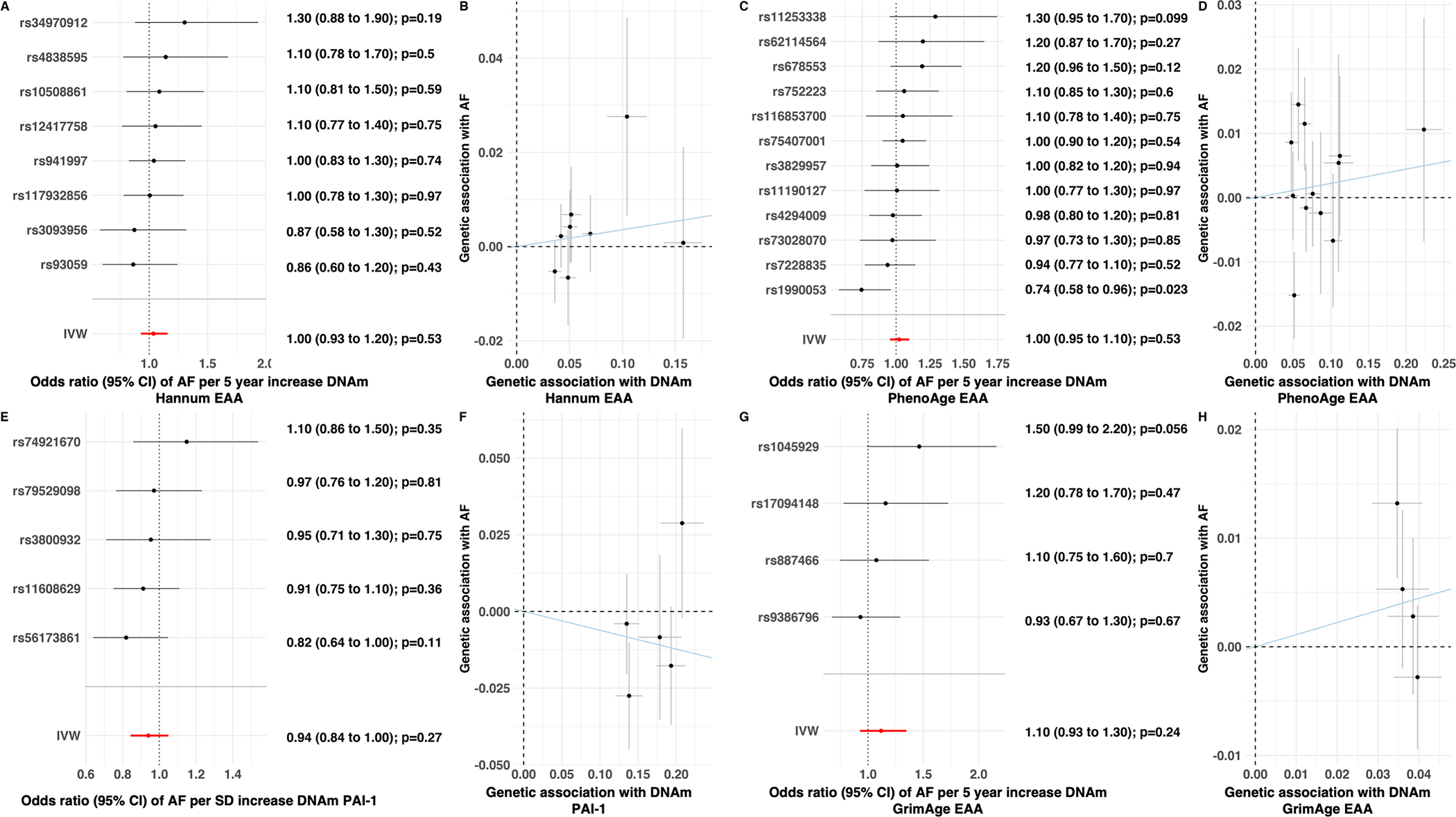
Methods: Measures for 4 epigenetic clocks (Horvath, Hannum, DNA methylation [DNAm] PhenoAge, and DNAm GrimAge) and an epigenetic predictor of PAI-1 (plasminogen activator inhibitor-1) levels (ie, DNAm PAI-1) were determined for study participants from 3 population-based cohort studies. Cox models evaluated for associations with incident AF and results were combined via random-effects meta-analyses. Two-sample summary-level Mendelian randomization analyses evaluated for associations between genetic instruments of the EAA measures and AF.
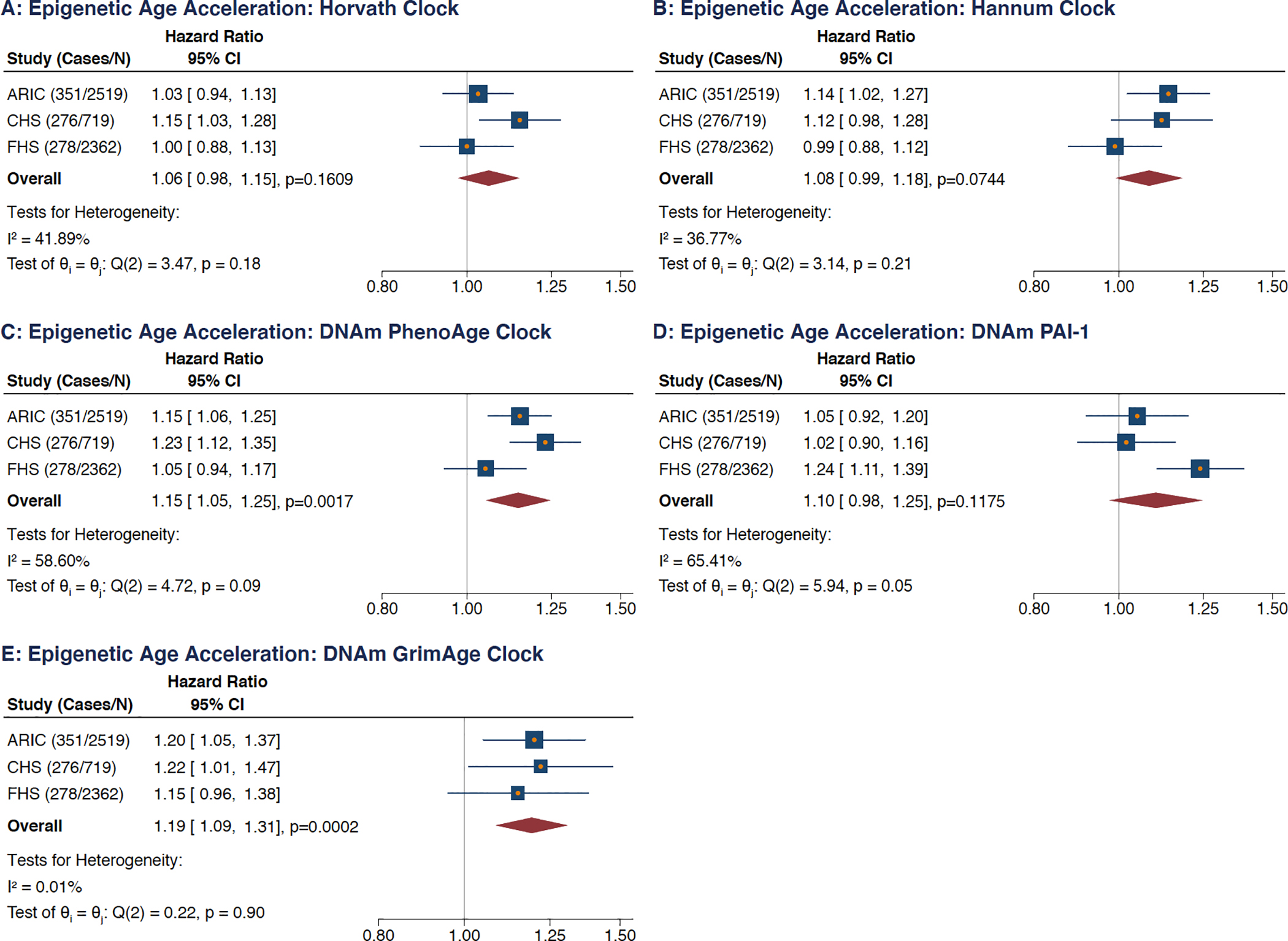
Results: Among 5600 participants (mean age, 65.5 years; female, 60.1%; Black, 50.7%), there were 905 incident AF cases during a mean follow-up of 12.9 years. Unadjusted analyses revealed all 4 epigenetic clocks and the DNAm PAI-1 predictor were associated with statistically significant higher hazards of incident AF, though the magnitudes of their point estimates were smaller relative to the associations observed for chronological age. The pooled EAA estimates for each epigenetic measure, with the exception of Horvath EAA, were associated with incident AF in models adjusted for chronological age, race, sex, and smoking variables. After multivariable adjustment for additional known AF risk factors that could also potentially function as mediators, pooled EAA measures for 2 clocks remained statistically significant. Five-year increases in EAA measures for DNAm GrimAge and DNAm PhenoAge were associated with 19% (adjusted hazard ratio [HR], 1.19 [95% CI, 1.09-1.31]; P<0.01) and 15% (adjusted HR, 1.15 [95% CI, 1.05-1.25]; P<0.01) higher hazards of incident AF, respectively. Mendelian randomization analyses for the 5 EAA measures did not reveal statistically significant associations with AF.
Conclusions: Our study identified adjusted associations between EAA measures and incident AF, suggesting that biological aging plays an important role independent of chronological age, though a potential underlying causal relationship remains unclear. These aging processes may be modifiable and not constrained by the immutable factor of time.
Keywords: aging; atrial fibrillation; epigenomics; genetics.
Figures
Comment in
-
Accelerated Epigenetic Aging and Incident Atrial Fibrillation: New Outlook on an Immutable Risk Factor?Circulation. 2021 Dec 14;144(24):1912-1914. doi: 10.1161/CIRCULATIONAHA.121.057533. Epub 2021 Dec 13. Circulation. 2021. PMID: 34898242 Free PMC article. No abstract available.
References
-
- Heijman J, Guichard J-B, Dobrev D, Nattel S. Translational Challenges in Atrial Fibrillation. Circ Res. 2018;122:752–773. - PubMed
-
- Hamczyk MR, Nevado RM, Barettino A, Fuster V, Andrés V. Biological Versus Chronological Aging: JACC Focus Seminar. J Am Coll Cardiol. 2020;75:919–930. - PubMed
-
- Horvath S, Raj K. DNA methylation-based biomarkers and the epigenetic clock theory of ageing. Nat Rev Genet. 2018;19:371–384. - PubMed
Publication types
MeSH terms
Grants and funding
- RC2 HL102419/HL/NHLBI NIH HHS/United States
- R01 HL139731/HL/NHLBI NIH HHS/United States
- R01 HL120393/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- 16EIA26410001/AHA/American Heart Association-American Stroke Association/United States
- R01 HL087652/HL/NHLBI NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- R01 HL128914/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- R01 HL103612/HL/NHLBI NIH HHS/United States
- N01 HC085080/HL/NHLBI NIH HHS/United States
- U01 AG060908/AG/NIA NIH HHS/United States
- U01 DK062413/DK/NIDDK NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- R01 NS087541/NS/NINDS NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- R01 HL105756/HL/NHLBI NIH HHS/United States
- K08 HL116640/HL/NHLBI NIH HHS/United States
- P30 DK063491/DK/NIDDK NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- K24 HL148521/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- 75N92019D00031/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- R01 HL141989/HL/NHLBI NIH HHS/United States
- R01 HL111089/HL/NHLBI NIH HHS/United States
- R01 HL116747/HL/NHLBI NIH HHS/United States
- R01 HL092111/HL/NHLBI NIH HHS/United States
