

Phenotypic Expression, Natural History, and Risk Stratification of Cardiomyopathy Caused by Filamin C Truncating Variants
- PMID: 34587765
- PMCID: PMC8595845
- DOI: 10.1161/CIRCULATIONAHA.121.053521
Phenotypic Expression, Natural History, and Risk Stratification of Cardiomyopathy Caused by Filamin C Truncating Variants
Abstract
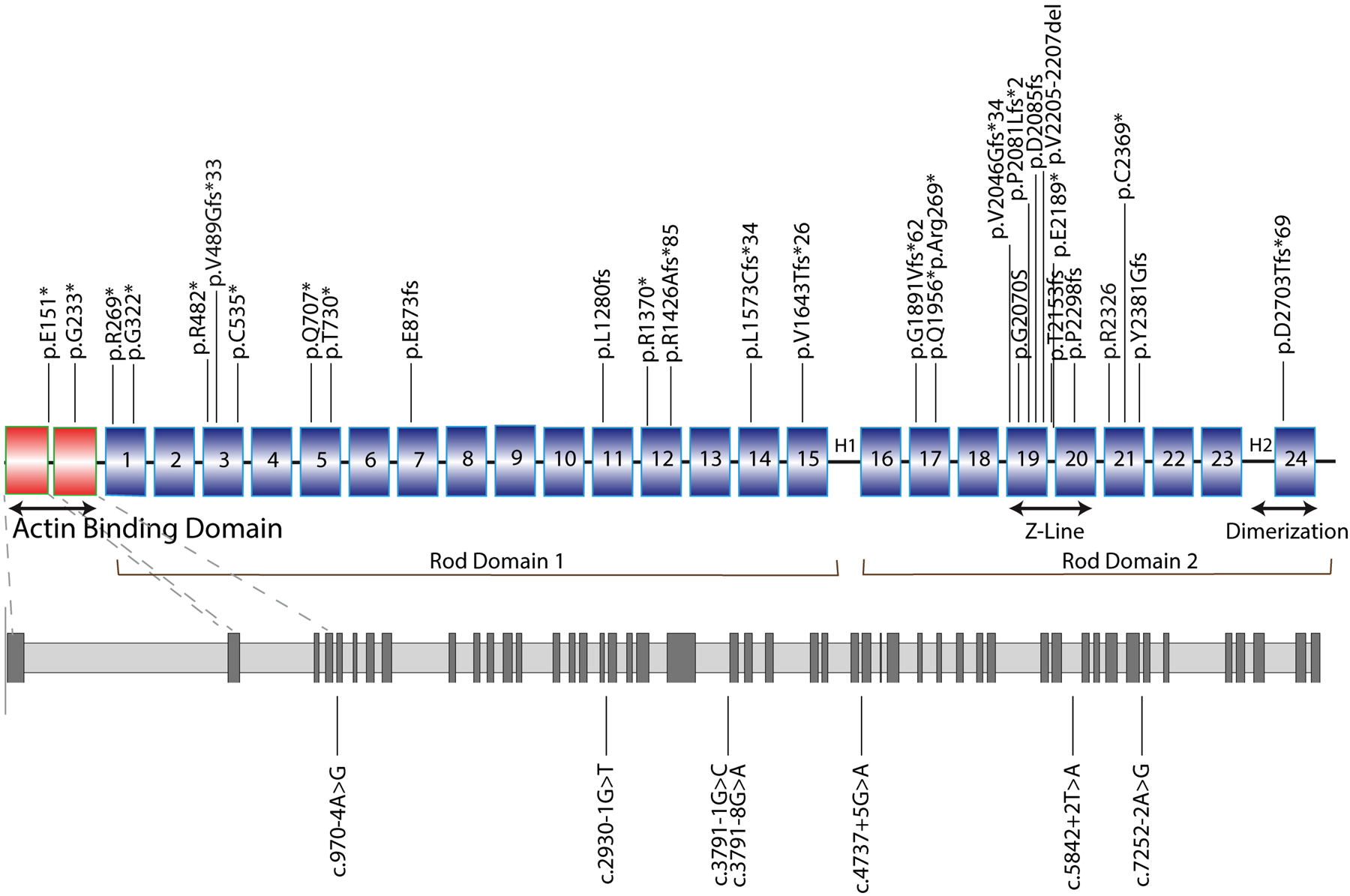
Background: Filamin C truncating variants (FLNCtv) cause a form of arrhythmogenic cardiomyopathy: the mode of presentation, natural history, and risk stratification of FLNCtv remain incompletely explored. We aimed to develop a risk profile for refractory heart failure and life-threatening arrhythmias in a multicenter cohort of FLNCtv carriers.
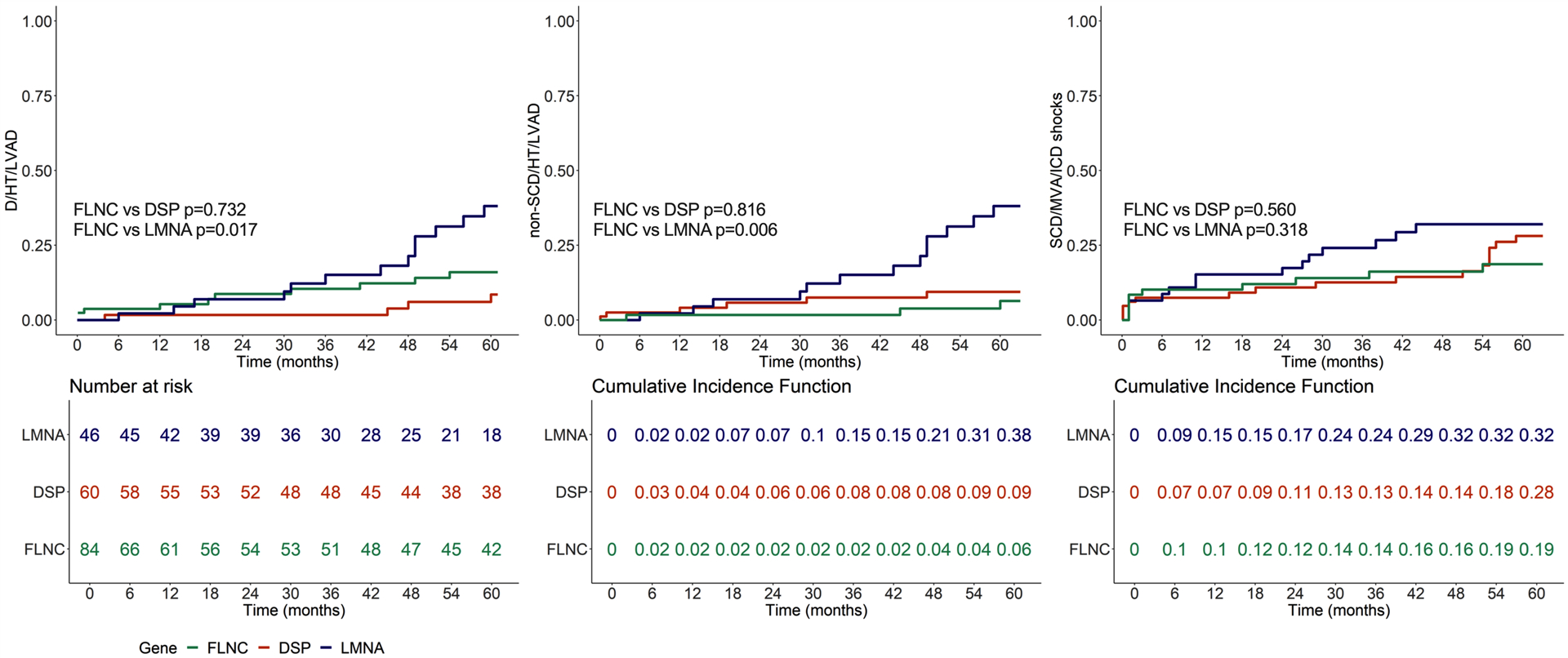
Methods: FLNCtv carriers were identified from 10 tertiary care centers for genetic cardiomyopathies. Clinical and outcome data were compiled. Composite outcomes were all-cause mortality/heart transplantation/left ventricle assist device (D/HT/LVAD), nonarrhythmic death/HT/LVAD, and sudden cardiac death/major ventricular arrhythmias. Previously established cohorts of 46 patients with LMNA and 60 with DSP-related arrhythmogenic cardiomyopathies were used for prognostic comparison.
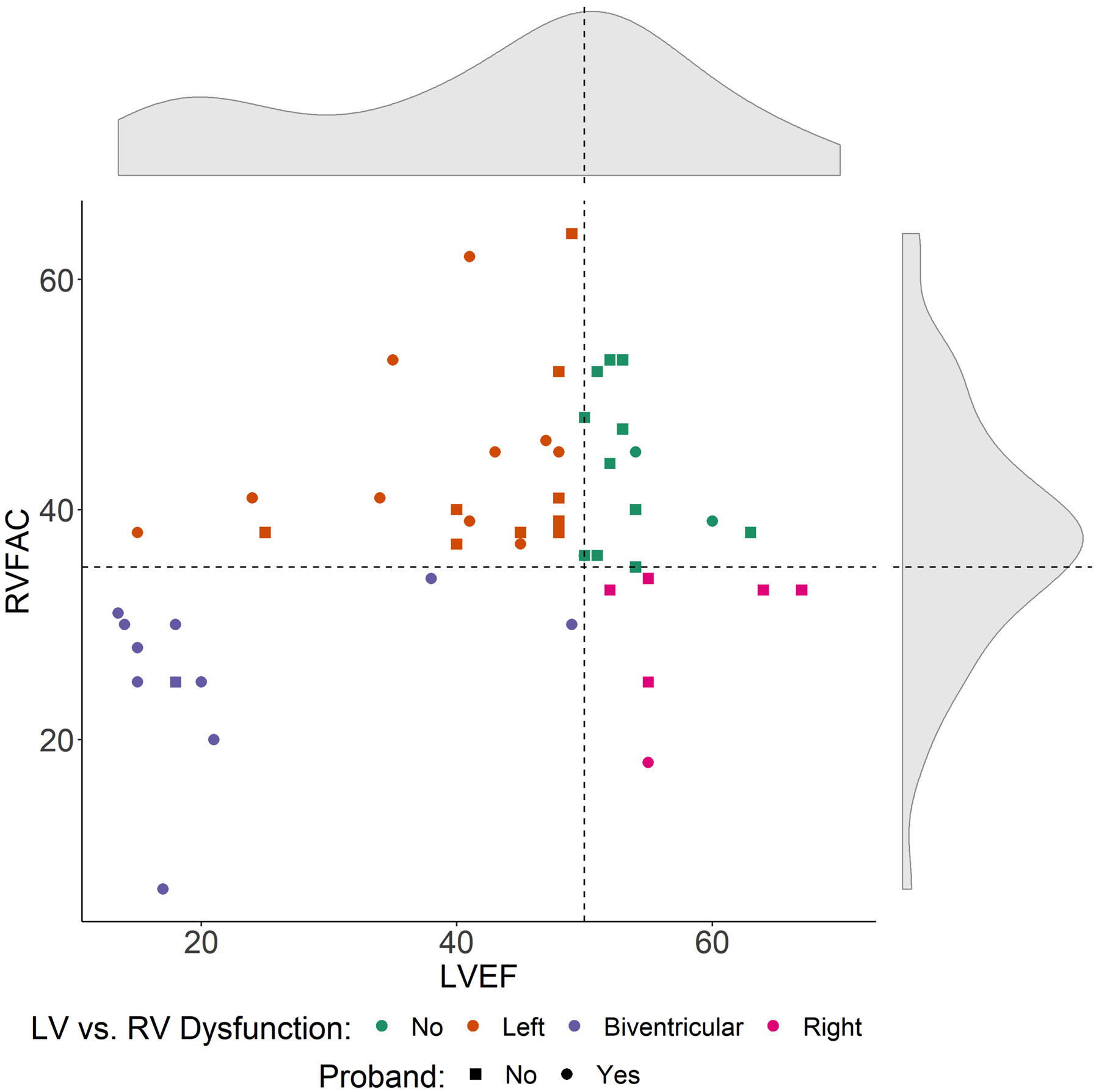
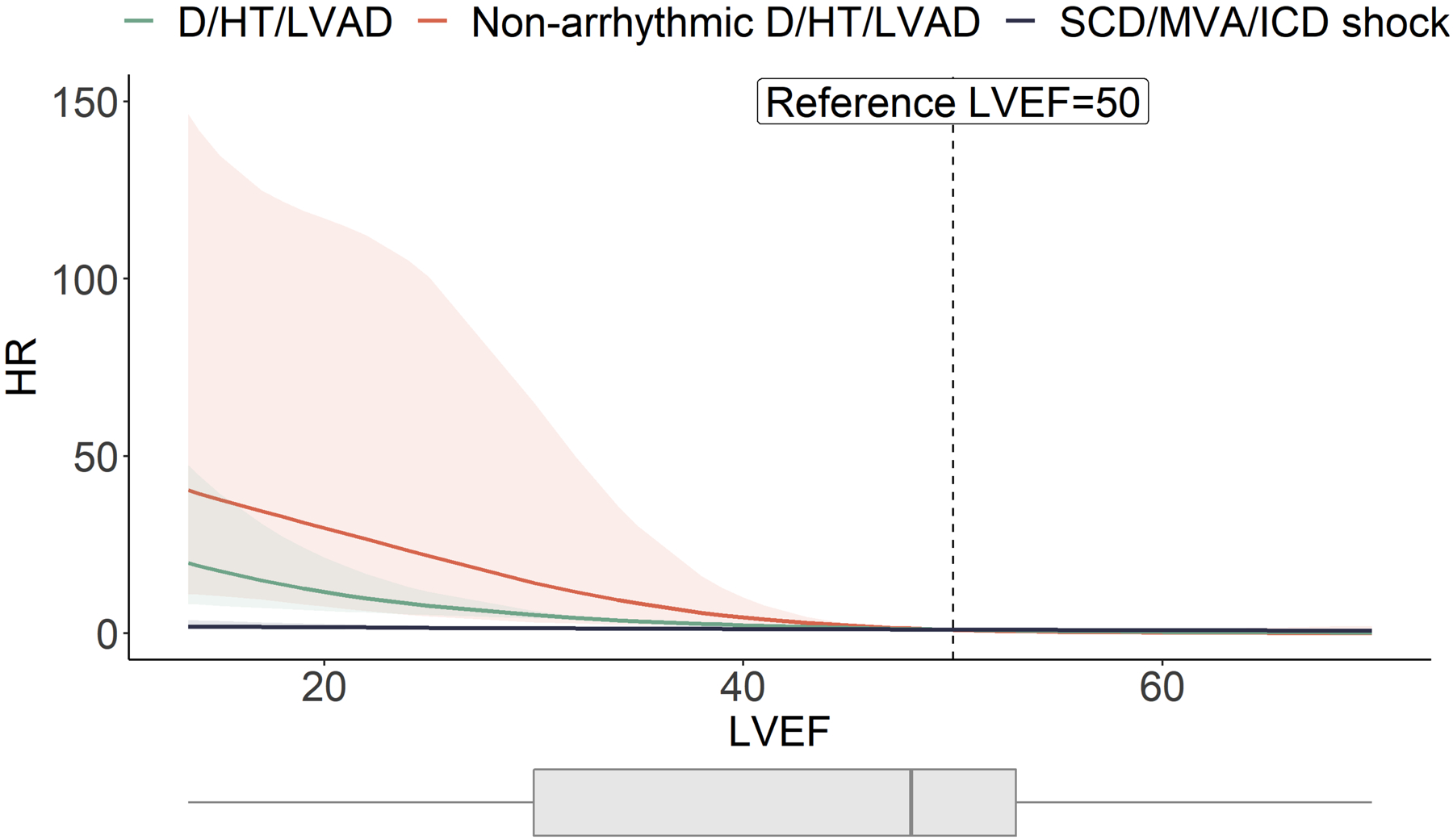
Results: Eighty-five patients carrying FLNCtv were included (42±15 years, 53% men, 45% probands). Phenotypes were heterogeneous at presentation: 49% dilated cardiomyopathy, 25% arrhythmogenic left dominant cardiomyopathy, 3% arrhythmogenic right ventricular cardiomyopathy. Left ventricular ejection fraction was <50% in 64% of carriers and 34% had right ventricular fractional area changes (RVFAC=(right ventricular end-diastolic area - right ventricular end-systolic area)/right ventricular end-diastolic area) <35%. During follow-up (median time 61 months), 19 (22%) carriers experienced D/HT/LVAD, 13 (15%) experienced nonarrhythmic death/HT/LVAD, and 23 (27%) experienced sudden cardiac death/major ventricular arrhythmias. The sudden cardiac death/major ventricular arrhythmias incidence of FLNCtv carriers did not significantly differ from LMNA carriers and DSP carriers. In FLNCtv carriers, left ventricular ejection fraction was associated with the risk of D/HT/LVAD and nonarrhythmic death/HT/LVAD.
Conclusions: Among patients referred to tertiary referral centers, FLNCtv arrhythmogenic cardiomyopathy is phenotypically heterogeneous and characterized by a high risk of life-threatening arrhythmias, which does not seem to be associated with the severity of left ventricular dysfunction.
Keywords: FLNC protein, human; arrhythmogenic right ventricular dysplasia; death, sudden, cardiac; heart failure; outcome studies; prognosis.
Figures
References
-
- Towbin JA, McKenna WJ, Abrams DJ, Ackerman MJ, Calkins H, Darrieux FCC, Daubert JP, de Chillou C, DePasquale EC, Desai MY, et al. 2019 HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy. Heart Rhythm. 2019;16:e301–e372. doi: 10.1016/j.hrthm.2019.05.007 - DOI - PubMed
-
- Spezzacatene A, Sinagra G, Merlo M, Barbati G, Graw SL, Brun F, Slavov D, Di Lenarda A, Salcedo EE, Towbin JA, et al. Arrhythmogenic Phenotype in Dilated Cardiomyopathy: Natural History and Predictors of Life-Threatening Arrhythmias. J Am Heart Assoc. 2015;4:e002149. doi: 10.1161/JAHA.115.002149 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL147064/HL/NHLBI NIH HHS/United States
- R01 HL109209/HL/NHLBI NIH HHS/United States
- UL1 TR002535/TR/NCATS NIH HHS/United States
- U01 HG007708/HG/NHGRI NIH HHS/United States
- UM1 HG006542/HG/NHGRI NIH HHS/United States
- R01 HL069071/HL/NHLBI NIH HHS/United States
- U24 EB023674/EB/NIBIB NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- K08 HL143185/HL/NHLBI NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- R01 HL116906/HL/NHLBI NIH HHS/United States
- 17GRNT33670495/AHA/American Heart Association-American Stroke Association/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
