

Predominant role of gut-vagus-brain neuronal pathway in postoperative nausea and vomiting: evidence from an observational cohort study
- PMID: 34587905
- PMCID: PMC8480048
- DOI: 10.1186/s12871-021-01449-9
Predominant role of gut-vagus-brain neuronal pathway in postoperative nausea and vomiting: evidence from an observational cohort study
Abstract
Background: Postoperative nausea and vomiting (PONV) as a clinically most common postoperative complication requires multimodal antiemetic medications targeting at a wide range of neurotransmitter pathways. Lacking of neurobiological mechanism makes this 'big little problem' still unresolved. We aim to investigate whether gut-vagus-brain reflex generally considered as one of four typical emetic neuronal pathways might be the primary mediator of PONV.
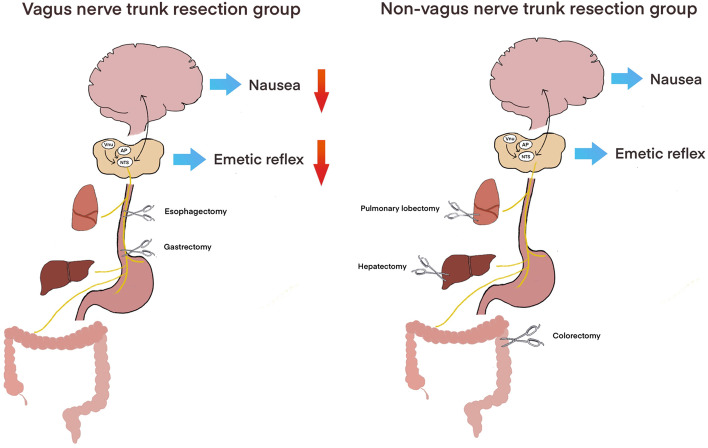
Methods: Three thousand two hundred twenty-three patients who underwent vagus nerve trunk resection (esophagectomy and gastrectomy) and non-vagotomy surgery (hepatectomy, pulmonary lobectomy and colorectomy) from December 2016 to January 2019 were enrolled. Thirty cases of gastrectomy with selective resection on the gastric branch of vagus nerve were also recruited. Nausea and intensity of vomiting was recorded within 24 h after the operation.
Results: PONV occurred in 11.9% of 1187 patients who underwent vagus nerve trunk resection and 28.7% of 2036 non-vagotomy patients respectively. Propensity score matching showed that vagotomy surgeries accounted for 19.9% of the whole PONV incidence, much less than that observed in the non-PONV group (35.1%, P < 0.01). Multivariate logistic regression result revealed that vagotomy was one of underlying factor that significantly involved in PONV (OR = 0.302, 95% CI, 0.237-0.386). Nausea was reported in 5.9% ~ 8.6% vagotomy and 12 ~ 17% non-vagotomy patients. Most vomiting were mild, being approximately 3% in vagotomy and 8 ~ 13% in non-vagotomy patients, while sever vomiting was much less experienced. Furthermore, lower PONV occurrence (10%) was also observed in gastrectomy undergoing selective vagotomy.
Conclusion: Patients undergoing surgeries with vagotomy developed less PONV, suggesting that vagus nerve dependent gut-brain signaling might mainly contribute to PONV.
Keywords: Emetic neuronal pathway; Postoperative nausea and vomiting; Vagotomy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Apfel C, Kranke P, Katz M, Goepfert C, Papenfuss T, Rauch S, Heineck R, Greim CA, Roewer N. Volatile anaesthetics may be the main cause of early but not delayed postoperative vomiting: a randomized controlled trial of factorial design. Br J Anaesth. 2002;88(5):659–668. doi: 10.1093/bja/88.5.659. - DOI - PubMed
-
- Hofer C, Zollinger A, Büchi S, Klaghofer R, Serafino D, Bühlmann S, Buddeberg C, Pasch T, Spahn D. Patient well-being after general anaesthesia: a prospective, randomized, controlled multi-centre trial comparing intravenous and inhalation anaesthesia. Br J Anaesth. 2003;91(5):631–637. doi: 10.1093/bja/aeg243. - DOI - PubMed
-
- Moore J, Elliott R, Payne K, Moore E, St Leger A, Harper N, Pollard B, Kerr J. The effect of anaesthetic agents on induction, recovery and patient preferences in adult day case surgery: a 7-day follow-up randomized controlled trial. Eur J Anaesthesiol. 2008;25(11):876–883. doi: 10.1017/S0265021507003493. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
