

Performance of acute respiratory distress syndrome definitions in a high acuity paediatric intensive care unit
- PMID: 34587946
- PMCID: PMC8480111
- DOI: 10.1186/s12931-021-01848-z
Performance of acute respiratory distress syndrome definitions in a high acuity paediatric intensive care unit
Abstract
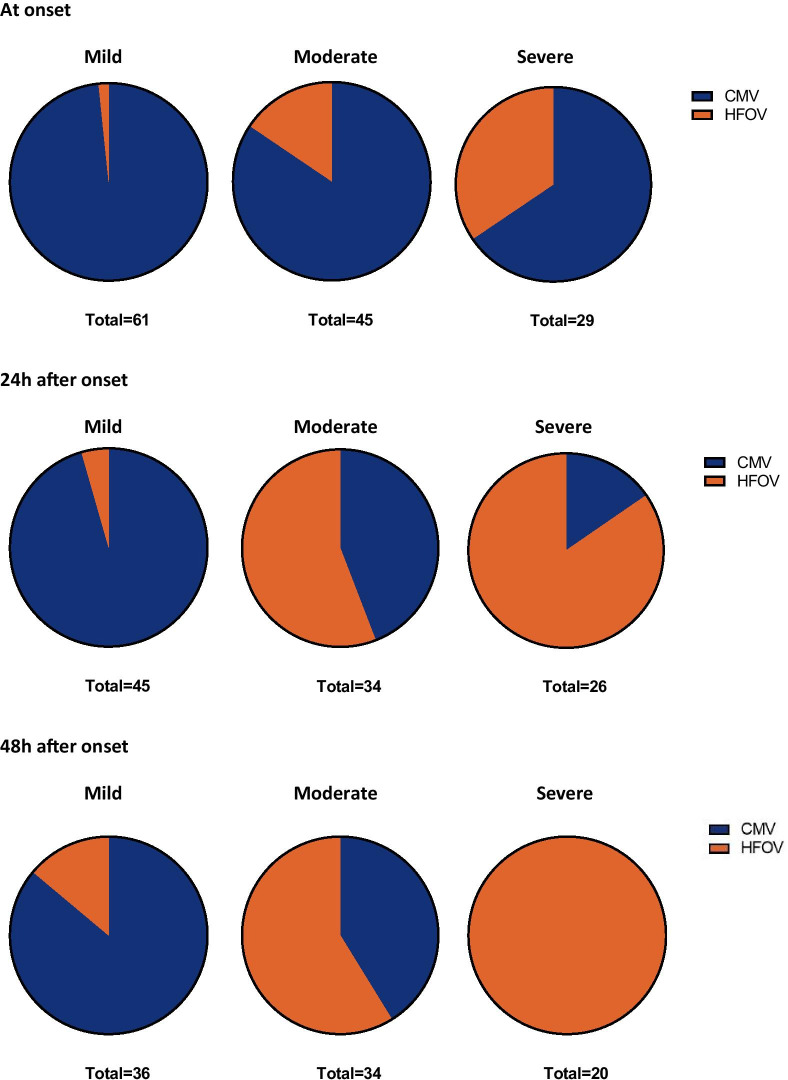
Background: For years, paediatric critical care practitioners used the adult American European Consensus Conference (AECC) and revised Berlin Definition (BD) for acute respiratory distress syndrome (ARDS) to study the epidemiology of paediatric ARDS (PARDS). In 2015, the paediatric specific definition, Paediatric Acute Lung Injury Consensus Conference (PALICC) was developed. The use of non-invasive metrics of oxygenation to stratify disease severity were introduced in this definition, although this potentially may lead to a confounding effect of disease severity since it is more common to place indwelling arterial lines in sicker patients. We tested the hypothesis that PALICC outperforms AECC/BD in our high acuity PICU, which employs a liberal use of indwelling arterial lines and high-frequency oscillatory ventilation (HFOV).
Methods: We retrospectively collected data from children < 18 years mechanically ventilated for at least 24 h in our tertiary care, university-affiliated paediatric intensive care unit. The primary endpoint was the difference in the number of PARDS cases between AECC/BD and PALICC. Secondary endpoints included mortality and ventilator free days. Performance was assessed by the area under the receiver operating characteristics curve (AUC-ROC).
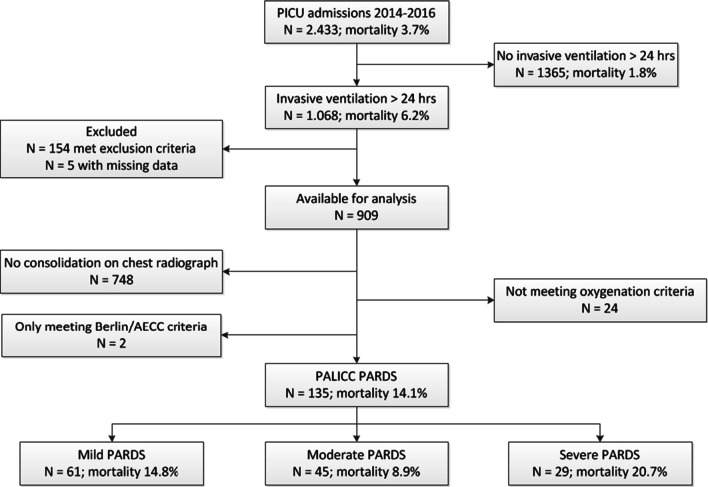
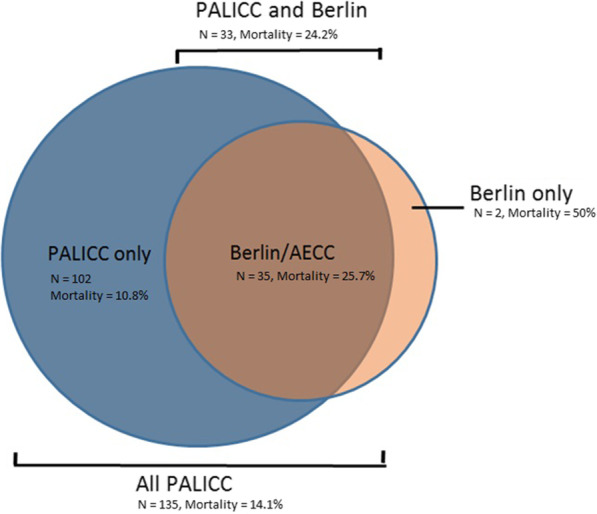
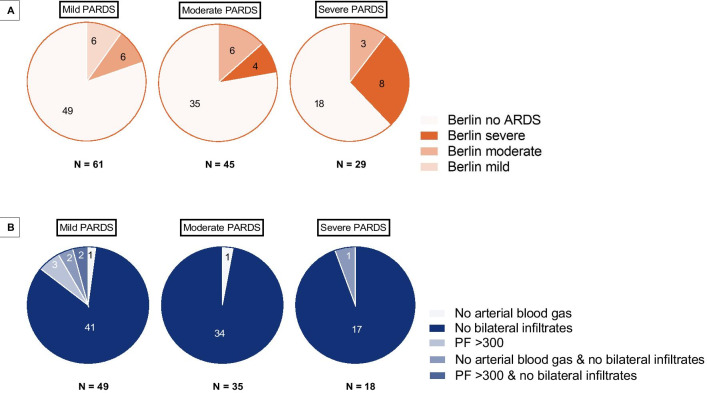
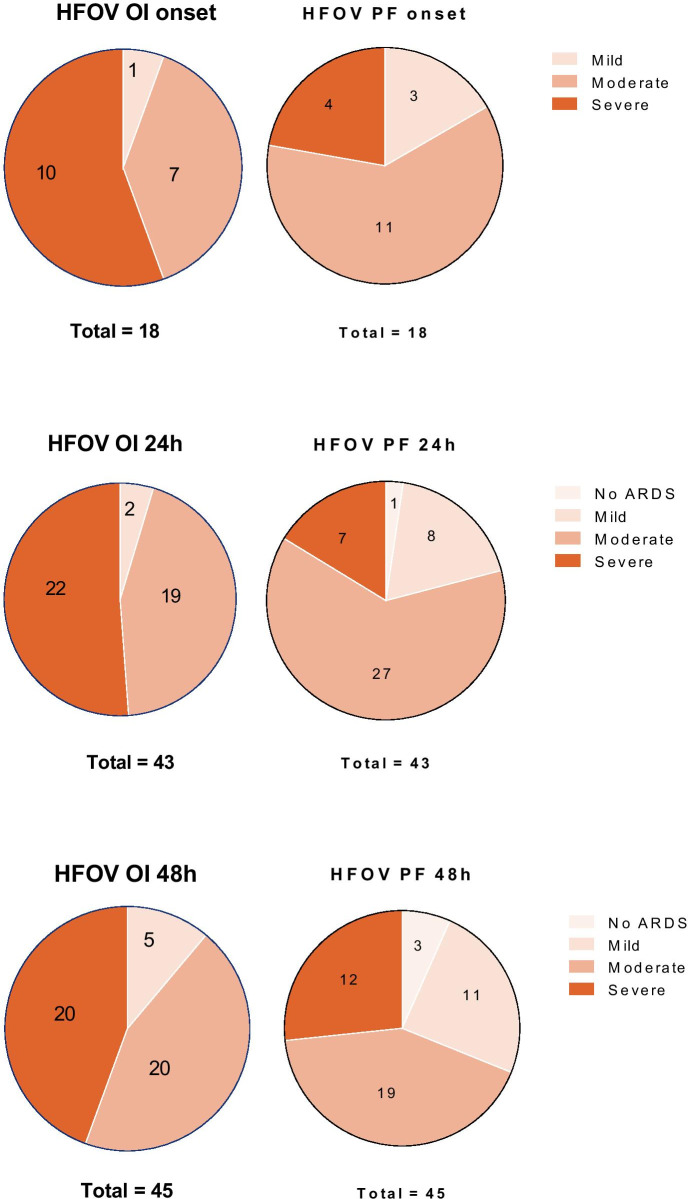
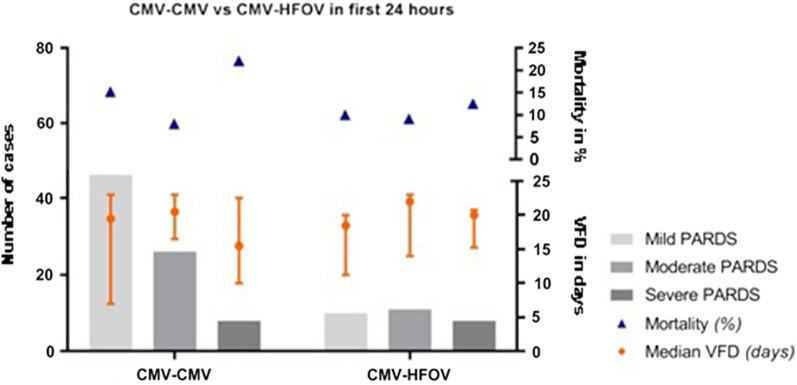
Results: Data from 909 out of 2433 patients was eligible for analysis. AECC/BD identified 35 (1.4%) patients (mortality 25.7%), whereas PALICC identified 135 (5.5%) patients (mortality 14.1%). All but two patients meeting AECC/Berlin criteria were also identified by PALICC. Almost half of the cohort (45.2%) had mild, 33.3% moderate and 21.5% severe PALICC PARDS at onset. Highest mortality rates were seen in patients with AECC acute lung injury (ALI)/mild Berlin and severe PALICC PARDS. The AUC-ROC for Berlin was the highest 24 h (0.392 [0.124-0.659]) after onset. PALICC showed the highest AUC-ROC at the same moment however higher than Berlin (0.531 [0.345-0.716]). Mortality rates were significantly increased in patients with bilateral consolidations (9.3% unilateral vs 26.3% bilateral, p = 0.025).
Conclusions: PALICC identified more new cases PARDS than the AECC/Berlin definition. However, both PALICC and Berlin performed poorly in terms of mortality risk stratification. The presence of bilateral consolidations was associated with a higher mortality rate. Our findings may be considered in future modifications of the PALICC criteria.
Keywords: Acute respiratory distress syndrome; American–European consensus conference; Berlin definition; Mechanical ventilation; Mortality; PICU; Paediatric; Paediatric acute lung injury consensus conference; Predictive value.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests in this section.
Figures
References
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, The American-European Consensus Conference on ARDS et al. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149(3 Pt 1):818–824. doi: 10.1164/ajrccm.149.3.7509706. - DOI - PubMed
-
- Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–2533. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
