

Predictors of outcomes in adults with acute myeloid leukemia and KMT2A rearrangements
- PMID: 34588432
- PMCID: PMC8481264
- DOI: 10.1038/s41408-021-00557-6
Predictors of outcomes in adults with acute myeloid leukemia and KMT2A rearrangements
Abstract
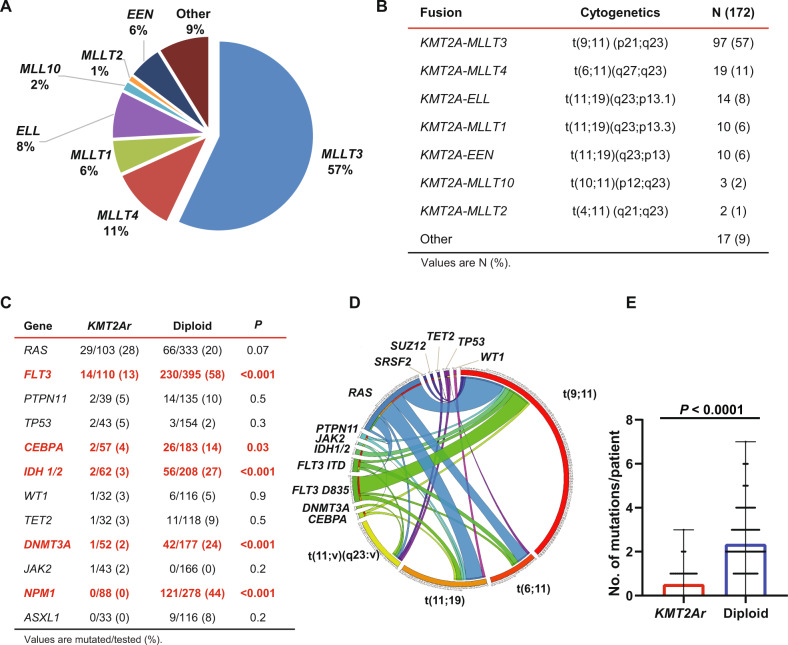
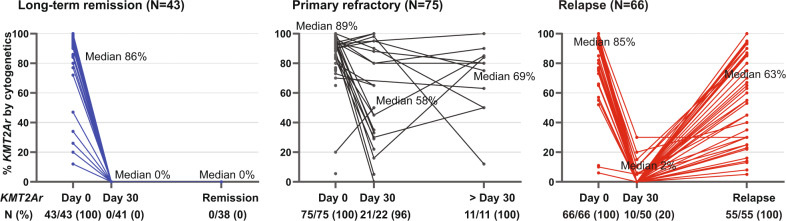
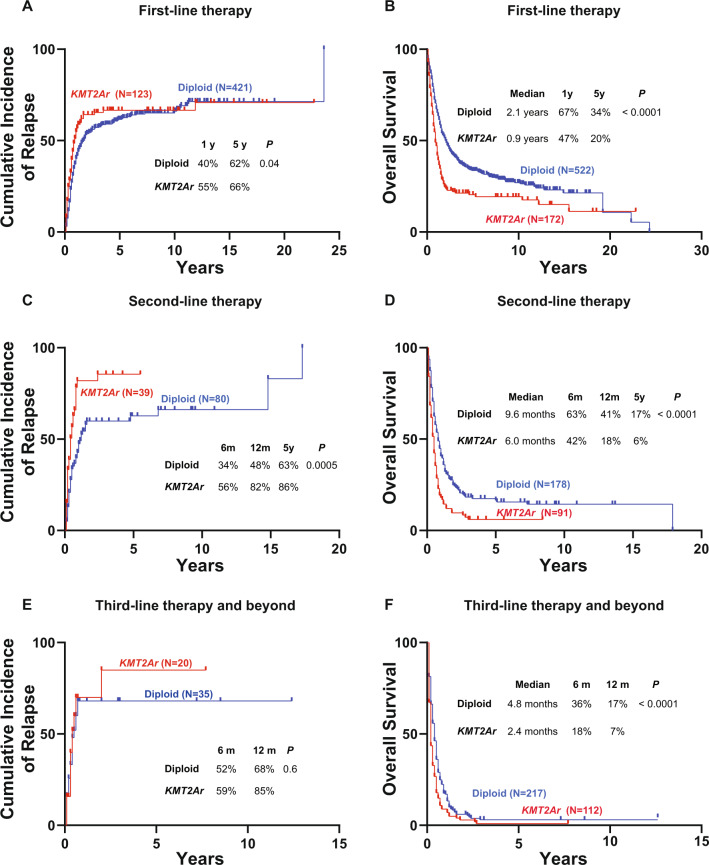
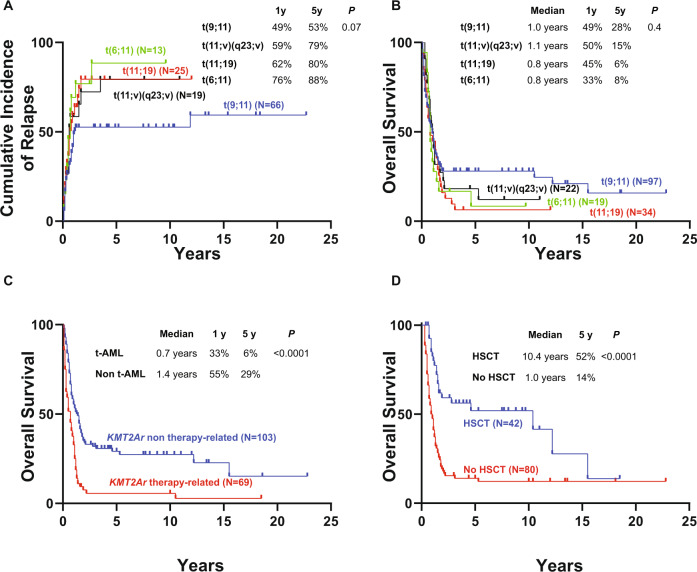
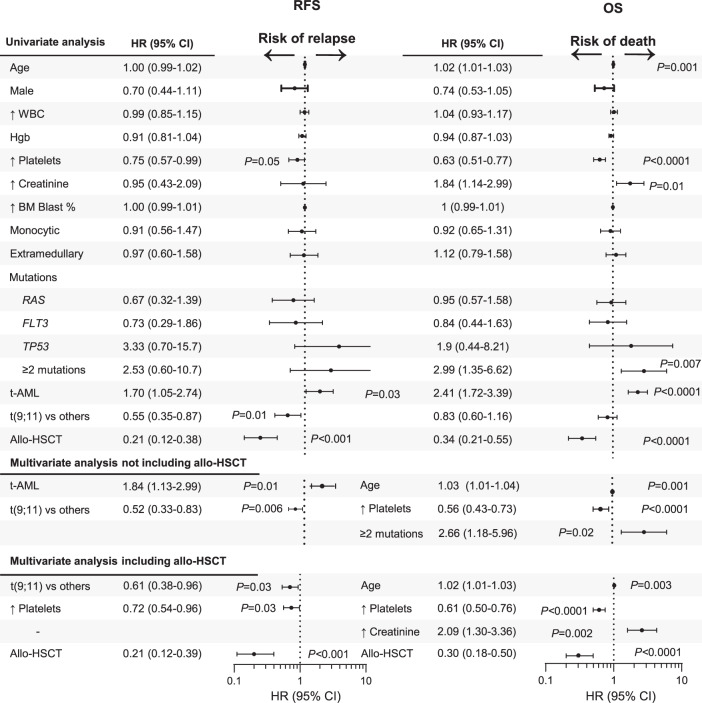
Acute myeloid leukemia (AML) with rearrangement of the lysine methyltransferase 2a gene (KMT2Ar) has adverse outcomes. However, reports on the prognostic impact of various translocations causing KMT2Ar are conflicting. Less is known about associated mutations and their prognostic impact. In a retrospective analysis, we identified 172 adult patients with KMT2Ar AML and compared them to 522 age-matched patients with diploid AML. KMT2Ar AML had fewer mutations, most commonly affecting RAS and FLT3 without significant impact on prognosis, except for patients with ≥2 mutations with lower overall survival (OS). KMT2Ar AML had worse outcomes compared with diploid AML when newly diagnosed and at relapse, especially following second salvage (median OS of 2.4 vs 4.8 months, P < 0.0001). Therapy-related KMT2Ar AML (t-AML) had worse outcomes compared with de novo KMT2Ar AML (median OS of 0.7 years vs 1.4 years, P < 0.0001). Allogeneic hematopoietic stem cell transplant (allo-HSCT) in first remission was associated with improved OS (5-year, 52 vs 14% for no allo-HSCT, P < 0.0001). In a multivariate analysis, translocation subtypes causing KMT2Ar did not predict survival, unlike age and allo-HSCT. In conclusion, KMT2Ar was associated with adverse outcomes regardless of translocation subtype. Therefore, AML risk stratification guidelines should include all KMT2Ar as adverse.
© 2021. The Author(s).
Conflict of interest statement
G.C.I. received research funding from Celgene, Kura Oncology, Syndax, and Novartis, and received consultancy fees from Novartis and Kura Oncology. K.S. received research funding from Novartis and consulting or advisory fees from Otsuka, Novartis, Pfizer, and Takeda. N.J.S. has served as a consultant for Takeda Oncology, AstraZeneca, and Jazz Pharmaceuticals, reports receiving research grants from Takeda Oncology and Astellas Pharma Inc. and has received honoraria from Amgen. C.D.D. received research funding from Abbvie, Agios, Calithera, Cleave, BMS/Celgene, Daiichi-Sankyo, Forma, ImmuneOnc, Loxo, and received consultancy or advisory board fees from AbbVie, Agios, Novartis, Aprea, Celgene/BMS, ImmuneOnc, Notable Laboratories, and Takeda. E.J. received research funding from Abbvie, Adaptive Biotechnologies, Amgen, Bristol Myers Squibb, Pfizer, and Takeda and received advisory board fees from Genetech. N.D. has received research funding from Daiichi-Sankyo, Bristol Myers Squibb, Pfizer, Gilead, Sevier, Genentech, Astellas, Abbvie, Hanmi, Trovagene, FATE therapeutics, Amgen, Novimmune, Glycomimetics, Trillium, and ImmunoGen and has served in a consulting or advisory role for Daiichi-Sankyo, Bristol Myers Squibb, Arog, Pfizer, Novartis, Jazz, Celgene, AbbVie, Astellas, Genentech, Immunogen, Servier, Syndax, Trillium, Gilead, Amgen, Shattuck Labs, and Agios. T.K. has received research funding from Bristol Myers Squibb, Celgene, Sanofi, Amgen, BiolineRx, Incyte, Genentech/AbbVie, Pfizer, Jazz Pharmaceuticals, AstraZeneca, Astellas Pharma, Ascentage Pharma, Genfleet, Cyclacel and received consulting or advisory board fees from Novartis, Jazz Pharmaceuticals, Pfizer, AbbVie/Genentech, and Agios. G.B. has received research funding from Incyte, GlaxoSmithKline, Cyclacel, BiolineRx, MedImmune, Lilly, Oncoceutics, Ryvu Therapeutics, Janssen Scientific Affairs, Bristol Myers Squibb, AbbVie, Novartis, AstraZeneca, Mundipharma Research, PTC Therapeutics, BioTheryX, XBiotech, Arvinas, Astex Pharmaceuticals, TCR2 Therapeutics, Nkarta, Treadwell Therapeutics, Cellestia Biotech, and consulting or advisory board fees from Argenx, PTC Therapeutics, BiolineRx, BioTheryX, Nkarta, Treadwell Therapeutics, Novartis, Catamaran Bio, and Takeda. G.G.-M. received research funding from Celgene, Astex Pharmaceuticals, Amphivena, Helsinn Therapeutics, Novartis, AbbVie, Bristol Myers Squibb, Onconova Therapeutics, H3 Biomedicine, Merck and consulting or advisory board fees from Celgene, Astex Pharmaceuticals, Acceleron Pharma, Helssin, and AbbVie. M.K. has received research funding from AbbVie, Genentech, Roche, Lilly, Cellectis, Calithera Biosciences, Ablynx, Agios, Ascentage Pharma, AstraZeneca, Sanofi and received honoraria or advisory board fees from AbbVie, Genentech, Roche, Amgen, Stemline Therapeutics, KisoJi Biotechnology, Stemline Therapeutics, Forty Seven, and Janssen. M.A. received research funding from Daiichi-Sankyo, and consultancy honoraria from Syndax, Jazz, Celgene, Amgen, AstraZeneca, Dimensions Capital, and equity ownership from Reata, Aptose, Europics, Senti Bio, Chimerix, and Oncolyze. H.M.K. received research funding from Ariad, Astex, Bristol Myers Squibb, Cyclacel, Daiichi-Sankyo, Pfizer, Immunogen, Jazz, Novartis and honoraria from Pfizer, Immunogen, Actinium, and Takeda. F.R. received research funding from Amgen, Bristol Myers Squibb, Sunesis Pharmaceuticals, Pfizer, Xenecor, Macrogenetics, Taiho, Astex, Abbvie and honoraria for consulting or advisory role from Jazz, Amgen, Celgene, Astellas, Syros, Taiho, Novartis, AstraZeneca, Agios, and Bristol Myers Squibb.
Figures
References
-
- Byrd JC, Mrózek K, Dodge RK, Carroll AJ, Edwards CG, Arthur DC, et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461) Blood. 2002;100:4325–36. doi: 10.1182/blood-2002-03-0772. - DOI - PubMed
-
- Grimwade D, Hills RK, Moorman AV, Walker H, Chatters S, Goldstone AH, et al. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood. 2010;116:354–65. doi: 10.1182/blood-2009-11-254441. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
