

Prevalence of elevated serum fatty acid synthase in chronic limb-threatening ischemia
- PMID: 34588500
- PMCID: PMC8481229
- DOI: 10.1038/s41598-021-98479-7
Prevalence of elevated serum fatty acid synthase in chronic limb-threatening ischemia
Abstract
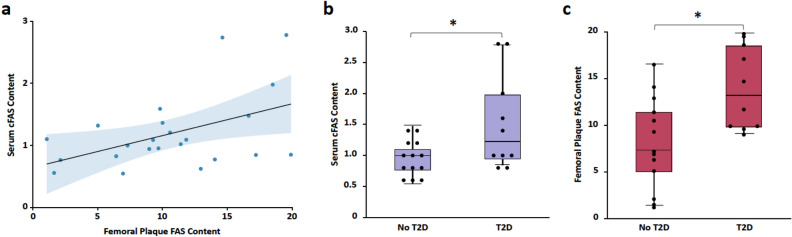
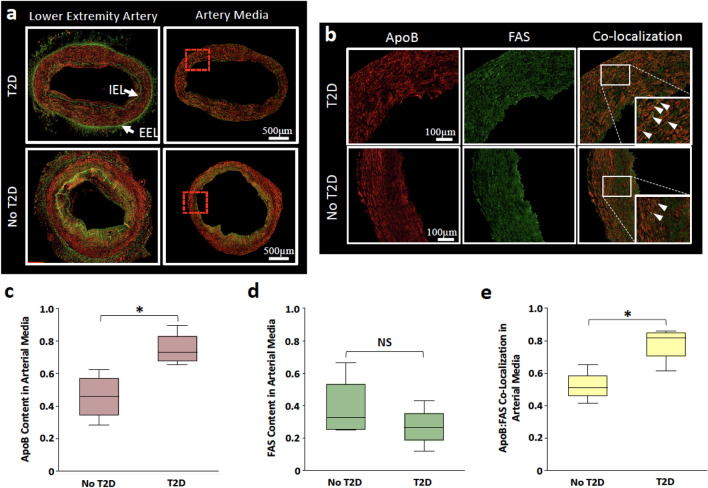
There are currently no serum-based evaluations that can corroborate the severity of peripheral artery disease (PAD). In this cross-sectional study, we assessed the prevalence of elevated serum fatty acid synthase (cFAS) in patients with chronic limb-threatening ischemia (CLTI) and evaluated the accuracy of its use in detecting this condition. Preoperative fasting serum samples from 87 patients undergoing vascular intervention were collected between October 2014 and September 2016. Median age was 62 years, with 56 (64%) men, and 32 (37%) with CLTI. We found that elevated cFAS content (OR 1.17; 95% CI 1.04-1.31), type 2 diabetes (T2D; OR 5.22; 95% CI 1.77-15.4), and smoking (OR 3.53; 95% CI 1.19-10.5) were independently associated with CLTI and could detect the presence of CLTI with 83% accuracy (95% CI 0.74-0.92). Furthermore, serum FAS content was positively correlated with FAS content in femoral artery plaque in patients with severe PAD ([Formula: see text] = 0.22; P = 0.023). Finally, significantly higher co-localization of FAS and ApoB were observed within lower extremity arterial media (P < .001). Our findings indicate that serum FAS content is a marker for disease severity in patients with PAD, independent of concomitant T2D and smoking, and may play a key role in FAS and ApoB peripheral plaque progression.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
