

Raising the bar to ultradisciplinary collaborations in management of chronic thromboembolic pulmonary hypertension
- PMID: 34589266
- PMCID: PMC8462103
- DOI: 10.5606/tgkdc.dergisi.2021.21284
Raising the bar to ultradisciplinary collaborations in management of chronic thromboembolic pulmonary hypertension
Abstract
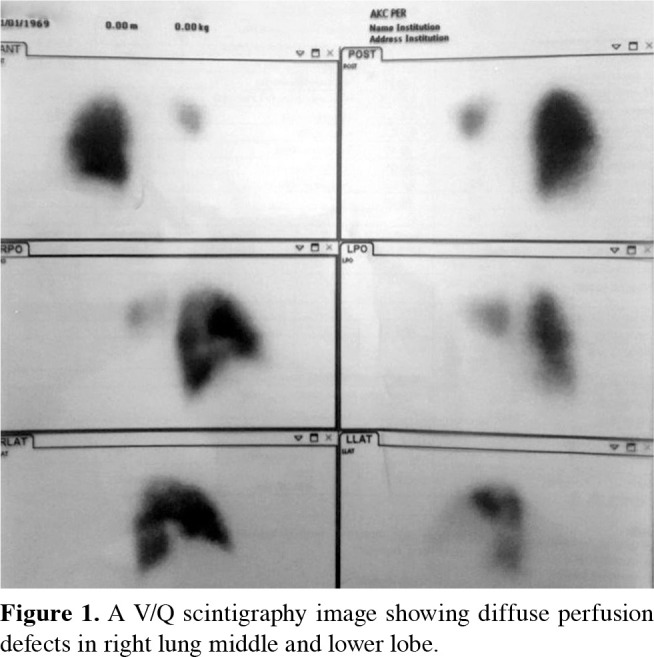
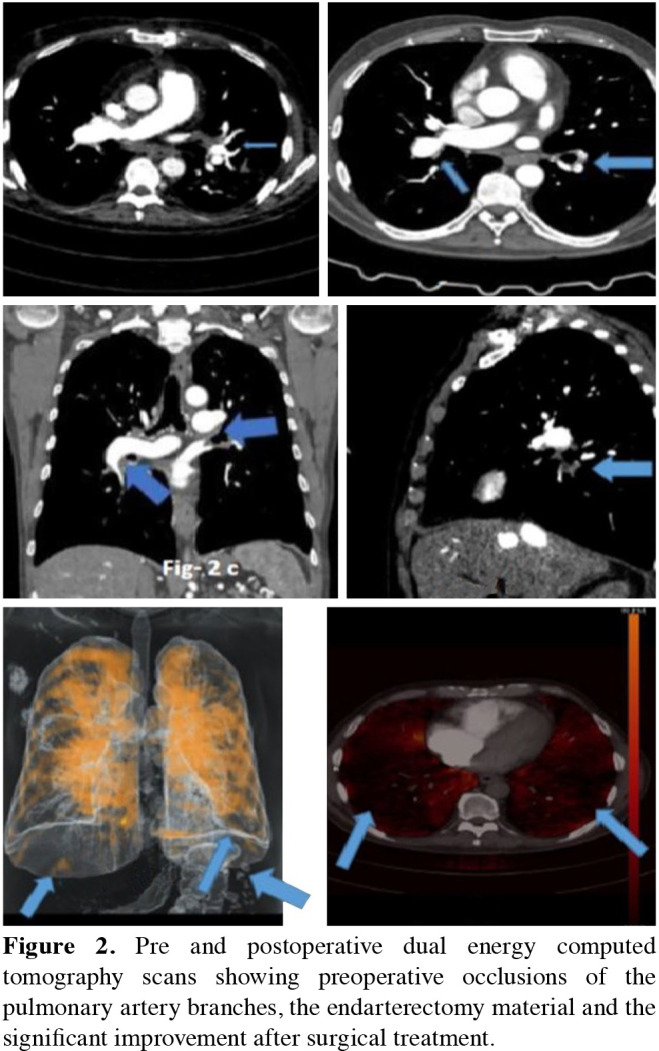
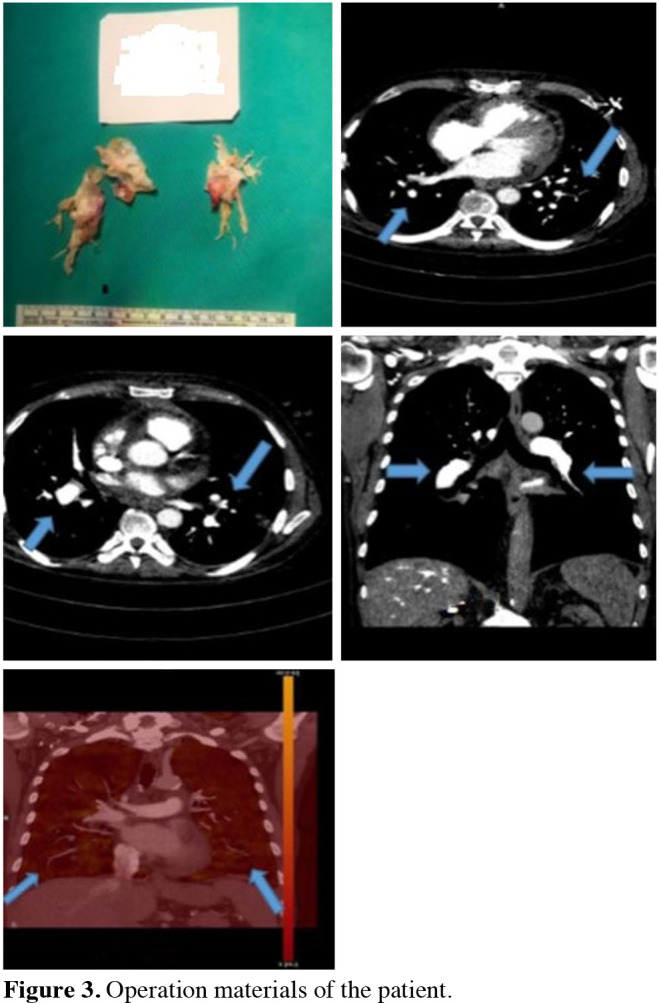
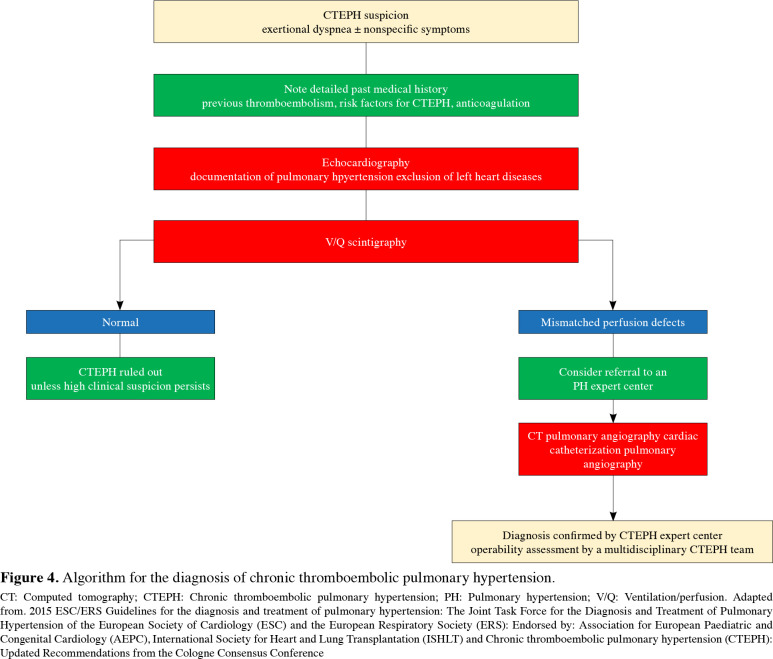
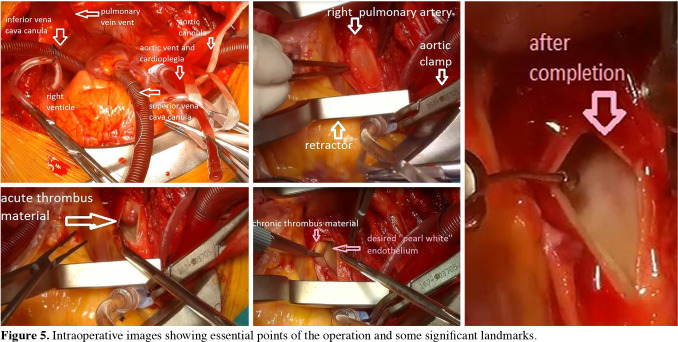
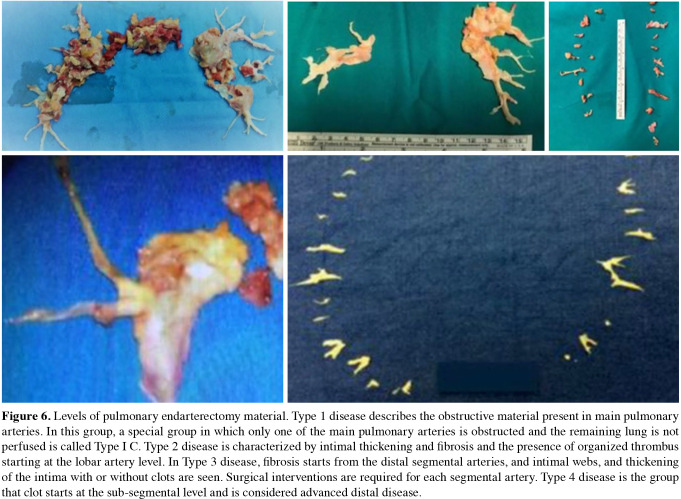
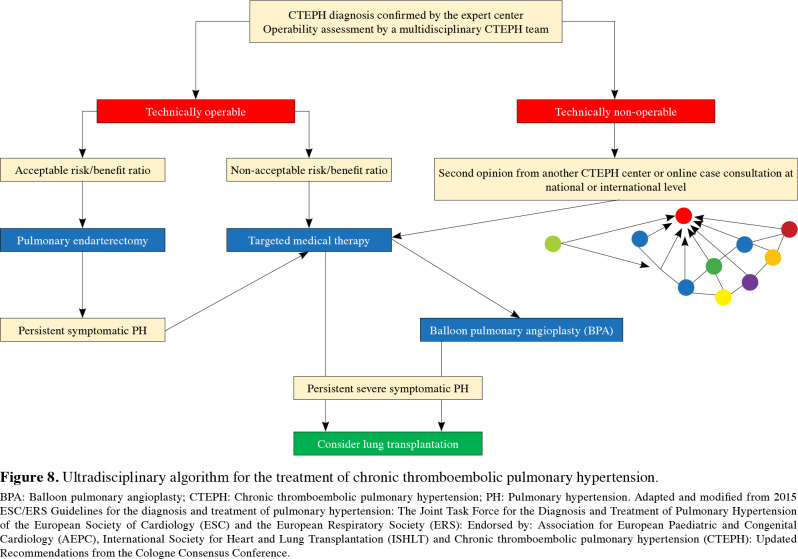
Chronic thromboembolic pulmonary hypertension is an underdiagnosed and potentially fatal subgroup of pulmonary hypertension, if left untreated. Clinical signs include exertional dyspnea and non-specific symptoms. Diagnosis requires multimodality imaging and heart catheterization. Pulmonary endarterectomy, an open heart surgery, is the gold standard treatment of choice in selected patients in specialized centers. Targeted medical therapy and balloon pulmonary angioplasty can be effective in high-risk patients with significant comorbidities, distal pulmonary vascular obstructions, or recurrent/persistent pulmonary hypertension after pulmonary endarterectomy. Currently, there is a limited number of data regarding novel coronavirus-2019 infection in patients with chronic thromboembolic pulmonary hypertension and the changing spectrum of the disease during the pandemic. Challenging times during this outbreak due to healthcare crisis and relatively higher case-fatality rates require convergence; that is an ultradisciplinary collaboration, which crosses disciplinary and sectorial boundaries to develop integrated knowledge and new paradigms. Management strategies for the "new normal" such as virtual care, preparedness for further threats, redesigned standards and working conditions, reevaluation of specific recommendations, and online collaborations for optimal decisions for chronic thromboembolic pulmonary hypertension patients may change the poor outcomes.
Keywords: Balloon pulmonary angioplasty; chronic thromboembolic pulmonary hypertension; pulmonary endarterectomy; pulmonary thromboembolism; targeted medical therapy.
Copyright © 2021, Turkish Society of Cardiovascular Surgery.
Conflict of interest statement
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Figures
References
-
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Respir J. 2015;46:903–975. - PubMed
-
- Wilkens H, Konstantinides S, Lang IM, Bunck AC, Gerges M, Gerhardt F, et al. Chronic thromboembolic pulmonary hypertension (CTEPH): Updated Recommendations from the Cologne Consensus Conference 2018. Int J Cardiol. 2018;272:69–78. - PubMed
-
- Taş SG. In: Damar. Polat A, Akay HT, Köksal C, Bozkurt AK, editors. İstanbul: Bayçınar Tıbbi Yayıncılık; 2019. Pulmoner hipertansiyon; pp. 663–676.
Publication types
LinkOut - more resources
Full Text Sources