

Association of Cardiotoxicity With Doxorubicin and Trastuzumab: A Double-Edged Sword in Chemotherapy
- PMID: 34589374
- PMCID: PMC8459919
- DOI: 10.7759/cureus.18194
Association of Cardiotoxicity With Doxorubicin and Trastuzumab: A Double-Edged Sword in Chemotherapy
Abstract
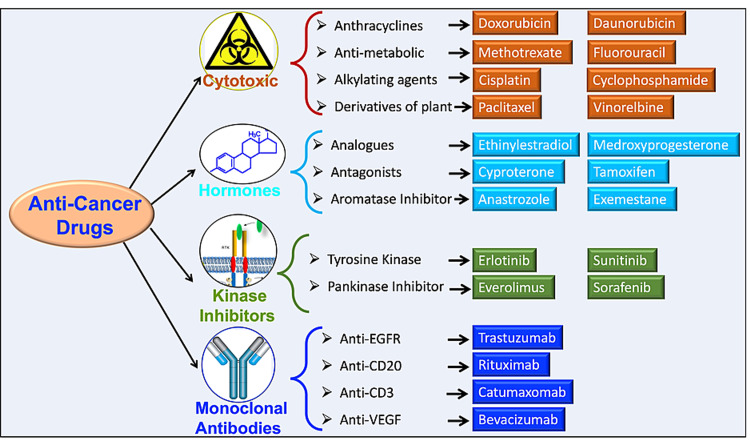
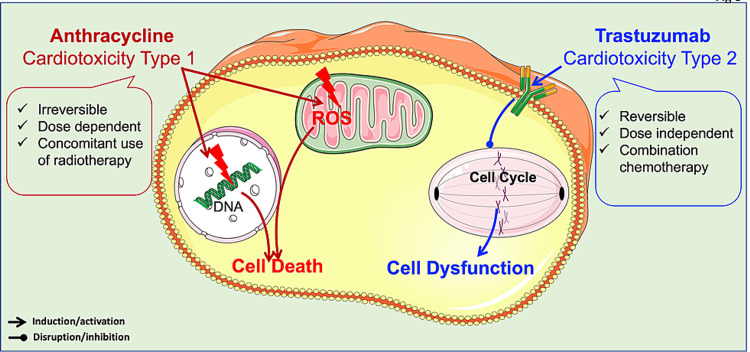
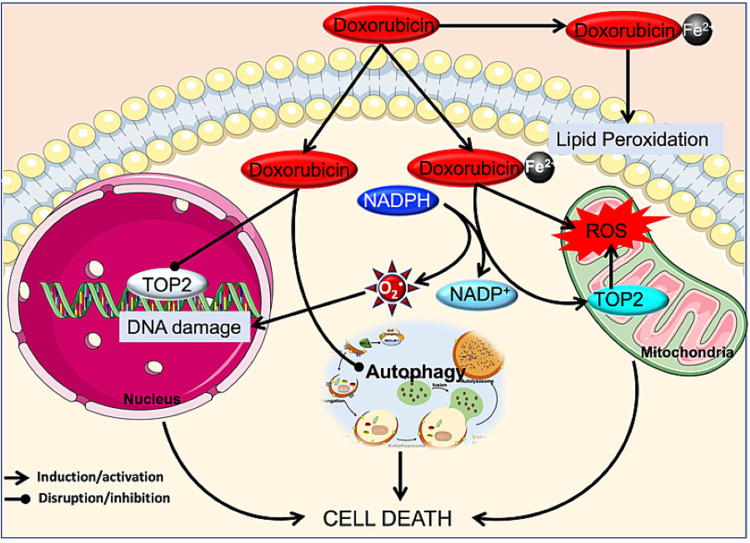
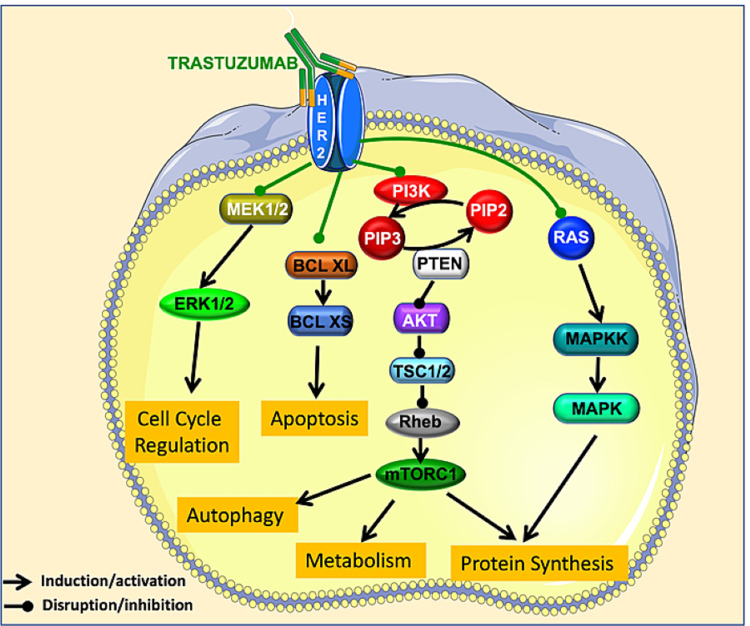
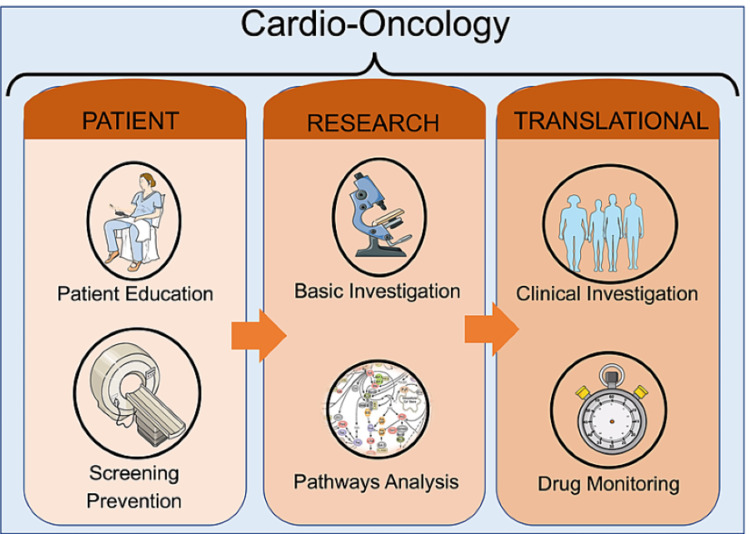
Anticancer drugs play an important role in reducing mortality rates and increasing life expectancy in cancer patients. Treatments include monotherapy and/or a combination of radiation therapy, chemotherapy, hormone therapy, or immunotherapy. Despite great advances in drug development, some of these treatments have been shown to induce cardiotoxicity directly affecting heart function and structure, as well as accelerating the development of cardiovascular disease. Such side effects restrict treatment options and can negatively affect disease management. Consequently, when managing cancer patients, it is vital to understand the mechanisms causing cardiotoxicity to better monitor heart function, develop preventative measures against cardiotoxicity, and treat heart failure when it occurs in this patient population. This review discusses the role and mechanism of major chemotherapy agents with principal cardiovascular complications in cancer patients.
Keywords: cancer; cardiotoxicity; chemotherapy; doxorubicin; trastuzumab.
Copyright © 2021, Gabani et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Cancer Statistics, 2017. Siegel RL, Miller KD, Jemal A. CA Cancer J Clin. 2017;67:7–30. - PubMed
-
- Clinical Cancer Advances 2018: annual report on progress against cancer from the American Society of Clinical Oncology. Heymach J, Krilov L, Alberg A, et al. J Clin Oncol. 2018;36:1020–1044. - PubMed
-
- [2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines] Zamorano JL, Lancellotti P, Muñoz DR, et al. Kardiol Pol. 2016;74:1193–1233. - PubMed
-
- Cardio-oncology: a new discipline in medicine to lead us into truly integrative care. Clarke E, Lenihan D. Future Cardiol. 2015;11:359–361. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources