

Management of a Unique Presentation of a Common Dermatologic Condition
- PMID: 34589664
- PMCID: PMC8405279
- DOI: 10.51894/001c.24501
Management of a Unique Presentation of a Common Dermatologic Condition
Abstract
Context: Skin rashes are a common complaint seen in the primary care setting. There are many dermatologic conditions which a primary care provider (PCP) should be able to recognize and manage. One such condition is granuloma annulare (GA), which commonly presents as smooth, annular plaques on the trunk and/or extremities. Rashes like GA rarely present as unique variants and may be difficult for PCPs to determine from patient history and physical exam alone. Patch granuloma annulare (patch GA) is an example that may clinically mimic a cutaneous lymphoma known as mycosis fungoides (MF). PCPs should ideally be able to recognize the utility of performing a skin biopsy and/or referring the patient to a dermatologist when history and physical exam alone are insufficient. The histologic findings of skin biopsies often become essential in establishing a proper diagnosis and guiding patient management in unique dermatologic variants.
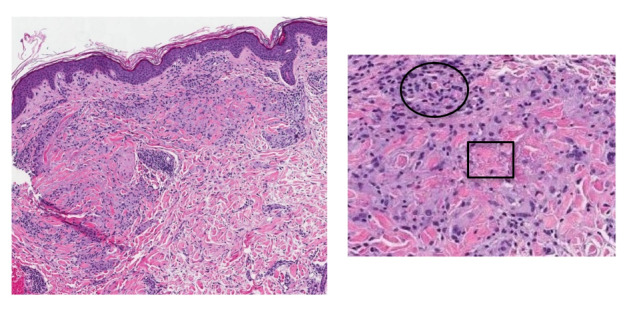
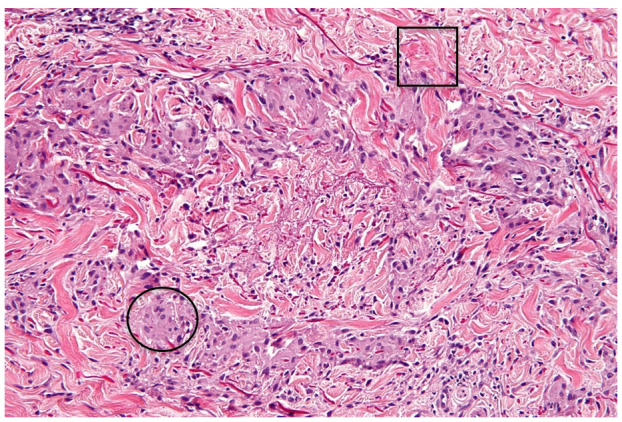
Example case: The patient in this clinical practice report is a Caucasian female in her late 60s who presented to a dermatology clinic with a two-year history of a worsening widespread eruption on her trunk and extremities. She had been evaluated previously by her PCP about 4 months prior and, without obtaining skin biopsies, treated her with a medium potency topical corticosteroid cream. The eruption had spread over her hips, buttocks, back, thighs, wrists, and elbows. Multiple skin biopsies of affected sites were taken by the second author and revealed findings consistent with patch GA. The patient was started on topical betamethasone dipropionate 0.05% ointment twice daily and noted marked improvement of her symptoms.
Conclusions: Although GA is a benign condition of the skin that may be readily detected by PCPs, skin biopsies may be necessary to establish a proper diagnosis when this condition presents as a unique variant (e.g., patch GA). Therapy for patch GA often begins with a trial of high-potency topical steroid therapy in combination with ultraviolet light exposure, depending on disease severity and patient preference. Early evaluation with a skin biopsy by her PCP or an earlier referral to a dermatologist to have skin biopsies performed likely would have helped establish a prompter diagnosis and treatment plan for this patient.
Keywords: biopsy; corticosteroid; granuloma annulare; macrophage; patch granuloma annulare; steroid.
Conflict of interest statement
None
Figures


Similar articles
-
Unusual Case of Granuloma Annulare Associated with Diabetes Mellitus.Acta Dermatovenerol Croat. 2020 Jul;28(1):45-46. Acta Dermatovenerol Croat. 2020. PMID: 32650853
-
Concomitant Subtypes of Granuloma Annulare in a 66-Year-Old Female: A Case Report.Cureus. 2023 Sep 26;15(9):e46026. doi: 10.7759/cureus.46026. eCollection 2023 Sep. Cureus. 2023. PMID: 37900443 Free PMC article.
-
Granuloma annulare and possible relation to purified protein derivative administration: a case report.J Med Case Rep. 2024 Jun 20;18(1):299. doi: 10.1186/s13256-024-04598-w. J Med Case Rep. 2024. PMID: 38902812 Free PMC article.
-
Evolution of granuloma annulare to mid-dermal elastolysis: report of a case and review of the literature.J Cutan Pathol. 2014 May;41(5):462-8. doi: 10.1111/cup.12292. Epub 2014 Feb 27. J Cutan Pathol. 2014. PMID: 24447045 Review.
-
Diagnosis and management of granuloma annulare.Am Fam Physician. 2006 Nov 15;74(10):1729-34. Am Fam Physician. 2006. PMID: 17137003 Review.
References
-
- Primary Care Providers as Allies in Dermatology. Beroukhim K., Danesh M., Nguyen C., Wu J.J., Koo J. Sep;2015 Practical Dermatology. :38–40.
LinkOut - more resources
Full Text Sources