

Management of pancreatic cysts and guidelines: what the gastroenterologist needs to know
- PMID: 34589706
- PMCID: PMC8474323
- DOI: 10.1177/26317745211045769
Management of pancreatic cysts and guidelines: what the gastroenterologist needs to know
Abstract
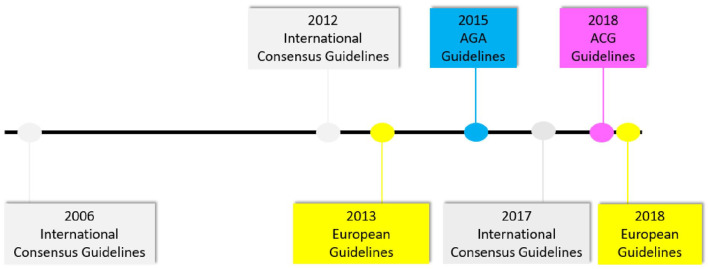
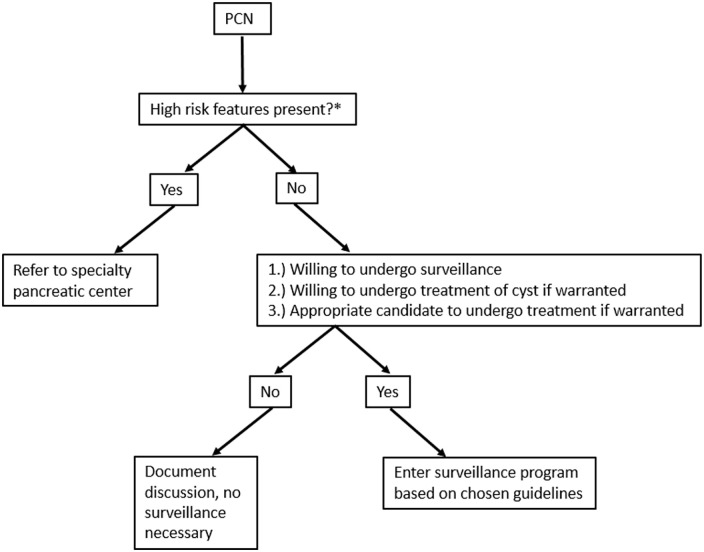
The prevalence of pancreatic cysts has increased significantly over the last decade, partly secondary to increased quality and frequency of cross-sectional imaging. While the majority never progress to cancer, a small number will and need to be followed. The management of pancreatic cysts can be both confusing and intimidating due to the multiple guidelines with varying recommendations. Despite the differences in the specifics of the guidelines, they all agree on several high-risk features that should get the attention of any clinician when assessing a pancreatic cyst: presence of a mural nodule or solid component, dilation of the main pancreatic duct (or presence of main duct intraductal papillary mucinous neoplasm), pancreatic cyst size ⩾3-4 cm, or positive cytology on pancreatic cyst fluid aspiration. Other important criteria to consider include rapid cyst growth (⩾5 mm/year), elevated serum carbohydrate antigen 19-9 levels, new-onset diabetes mellitus, or acute pancreatitis thought to be related to the cystic lesion.
Keywords: mucinous cystic neoplasms; pancreatic cyst; pancreatic cyst guidelines; pancreatic cystic neoplasms; pancreatic cystic tumors; pancreatic neoplasia.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vanessa M Shami is consultant for both Interpace Diagnostics and Olympus America. Ross CD Buerlein has no conflicts of interest.
Figures

References
-
- Kromrey ML, Bülow R, Hübner J, et al. Prospective study on the incidence, prevalence and 5-year pancreatic-related mortality of pancreatic cysts in a population-based study. Gut 2018; 67: 138–145. - PubMed
-
- Stark A, Donahue TR, Reber HA, et al. Pancreatic cyst disease: a review. JAMA 2016; 315: 1882–1893. - PubMed
-
- Tada M, Kawabe T, Arizumi M, et al. Pancreatic cancer in patients with pancreatic cystic lesions: a prospective study in 197 patients. Clin Gastroenterol Hepatol 2006; 4: 1265–1270. - PubMed
-
- Matsubara S, Tada M, Akahane M, et al. Incidental pancreatic cysts found by magnetic resonance imaging and their relationship with pancreatic cancer. Pancreas 2012; 41: 1241–1246. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
