

Development and Validation of a Simplified Prognostic Score in SCLC
- PMID: 34589918
- PMCID: PMC8474253
- DOI: 10.1016/j.jtocrr.2020.100016
Development and Validation of a Simplified Prognostic Score in SCLC
Abstract
Introduction: This study aimed at generating a new simplified prognostic score (SPS) using common clinical and biological variables to discriminate a limited number of subgroups of patients with SCLC differing by their overall survival (OS).
Methods: The SPS was developed exploring the Montpellier University Hospital retrospective database of 401 patients over a 16-year period. All patients had received etoposide - platinum-based chemotherapy as first-line treatment. The SPS development took into account significant determinants of OS in the Cox model, weighted by their regression β coefficients. Validation of the consequent SPS has been done separately in a combined population of 213 patients accrued from two different published trials (NCT03059667 and NCT00930891).
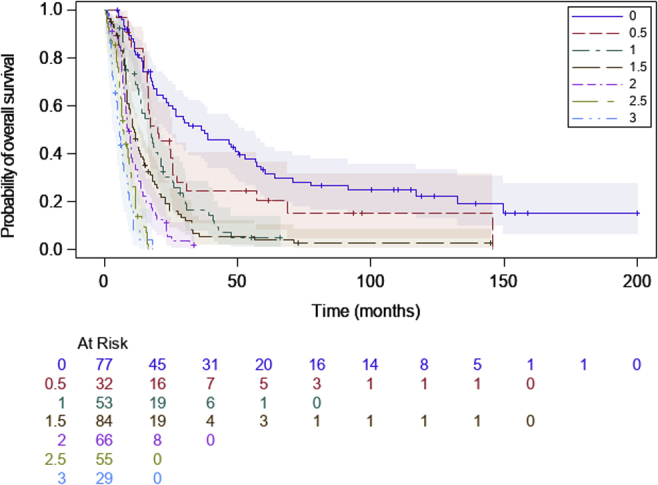
Results: The significant independent determinants of OS included the following: (1) American Joint Committee on Cancer TNM stage IV (hazard ratio [HR]: 2.52; 95% confidence interval [CI]: 1.91-3.33); (2) Eastern Cooperative Oncology Group performance status greater than 1 (HR: 2.27; 95% CI: 1.79-2.87); (3) the presence of liver metastases (HR: 1.66; 95% CI: 1.29-2.15); and (4) neutrophil-to-lymphocyte ratio greater than 4 (HR: 1.39; 95% CI: 1.11-1.92). The SPS generated with these four variables, segregated three groups (good, intermediate, and poor prognosis) with respective median OS of 26.9 months (95% CI: 20.1-38.9), 11.5 months (95% CI: 9.8-13.0), and 6.8 months (95% CI: 5.8-8.3; log-rank p < 10-4). Harrell's C statistic estimate was 0.68 ± 0.012, suggesting goodness of calibration. In the validation cohort, the SPS segregated the aforementioned three subgroups in a nearly similar manner, with respective median OS: 27.2, 12.3, and 8.6 months (log-rank p < 10-3; Harrell's C statistic: 0.58 ± 0.02).
Conclusions: The SPS is easy to calculate in real-life practice and efficiently discriminates three populations with different prognoses. This study deserves further validation of this score in patients with SCLC receiving immunochemotherapy.
Keywords: Chemotherapy; Prognosis; Prognostic score; Serum markers; Small cell lung cancer.
© 2020 The Authors.
Figures


References
-
- Arriagada R., Le Chevalier T., Pignon J.P. Initial chemotherapeutic doses and survival in patients with limited small-cell lung cancer. N Engl J Med. 1993;329:1848–1852. - PubMed
-
- Pujol J.L., Breton J.L., Gervais R. Phase III double-blind, placebo-controlled study of thalidomide in extensive-disease small-cell lung cancer after response to chemotherapy: an intergroup study FNCLCC cleo04 IFCT 00-01. J Clin Oncol. 2007;25:3945–3951. - PubMed
-
- Spigel D.R., Townley P.M., Waterhouse D.M. Randomized phase II study of bevacizumab in combination with chemotherapy in previously untreated extensive-stage small-cell lung cancer: results from the SALUTE trial. J Clin Oncol. 2011;29:2215–2222. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
