

Long-Term Recurrence of Completely Resected NSCLC
- PMID: 34589953
- PMCID: PMC8474471
- DOI: 10.1016/j.jtocrr.2020.100076
Long-Term Recurrence of Completely Resected NSCLC
Abstract
Introduction: The aim of this study is to evaluate the clinical backgrounds, including driver mutations, of those patients with early stage NSCLC who experienced recurrence beyond 5 years after complete resection.
Methods: We used a cohort of 512 consecutive cases of surgically resected NSCLC without other malignances from 2006 to 2011 in Aichi Cancer Center Hospital. The inclusion criteria for this cohort were patients with primary NSCLC who underwent a surgically curable operation.
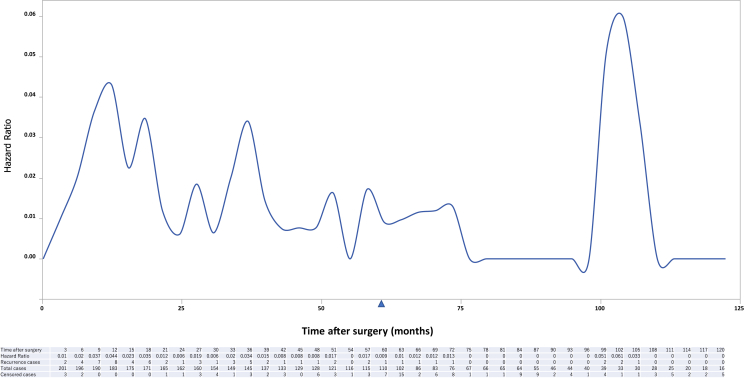
Results: A total of 172 patients (32.8%) had recurrence after the surgery. Among the recurrent cases, 17 patients (3.3%) had a relapse more than 5 years after the surgery, and all except one (16 of 17, 94.1%) had driver mutations, including gene rearrangements.
Conclusions: Even in early stage NSCLC after complete resection, it was found that some cases had a relapse more than 5 years after the surgery. Most of these cases had some kind of driver mutations; so more than 5 years of postoperative surveillance may be beneficial, especially in those with driver gene mutants.
Keywords: Driver mutation; Long-term recurrence; Non–small-cell lung cancer; Postoperative surveillance.
© 2020 The Authors.
Figures


References
-
- Solomon B.J., Mok T., Kim D.W. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371:2167–2177. - PubMed
-
- Calman L., Beaver K., Hind D., Lorigan P., Roberts C., Lloyd-Jones M. Survival benefits from follow-up of patients with lung cancer: a systematic review and meta-analysis. J Thorac Oncol. 2011;6:1993–2004. - PubMed
-
- Kosaka T., Yatabe Y., Onozato R., Kuwano H., Mitsudomi T. Prognostic implication of EGFR, KRAS, and TP53 gene mutations in a large cohort of Japanese patients with surgically treated lung adenocarcinoma. J Thorac Oncol. 2009;4:22–29. - PubMed
-
- Choi Y.L., Takeuchi K., Soda M. Identification of novel isoforms of the EML4-ALK transforming gene in non-small cell lung cancer. Cancer Res. 2008;68:4971–4976. - PubMed
-
- Fukui T., Yatabe Y., Kobayashi Y. Clinicoradiologic characteristics of patients with lung adenocarcinoma harboring EML4-ALK fusion oncogene. Lung Cancer. 2012;77:319–325. - PubMed
LinkOut - more resources
Full Text Sources
