

Earlier corticosteroid use for adverse event management in patients receiving axicabtagene ciloleucel for large B-cell lymphoma
- PMID: 34590303
- PMCID: PMC9293158
- DOI: 10.1111/bjh.17673
Earlier corticosteroid use for adverse event management in patients receiving axicabtagene ciloleucel for large B-cell lymphoma
Abstract
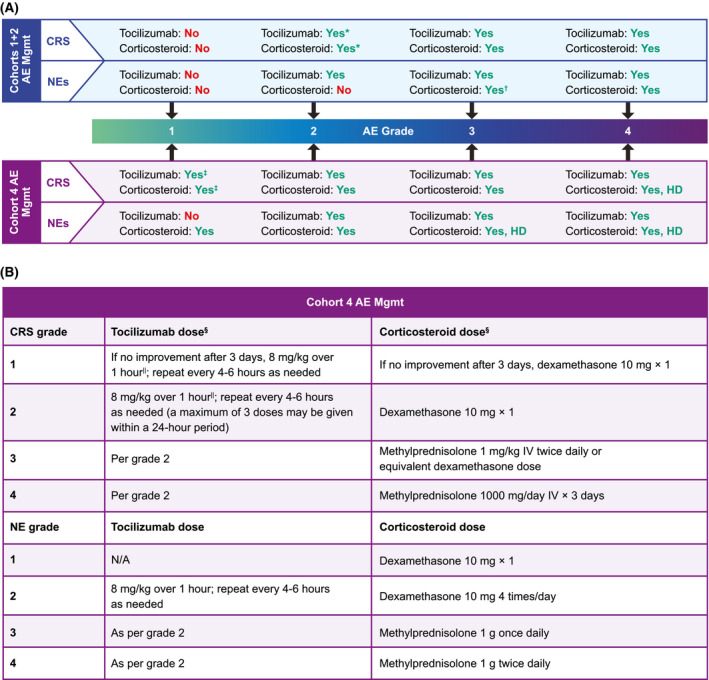
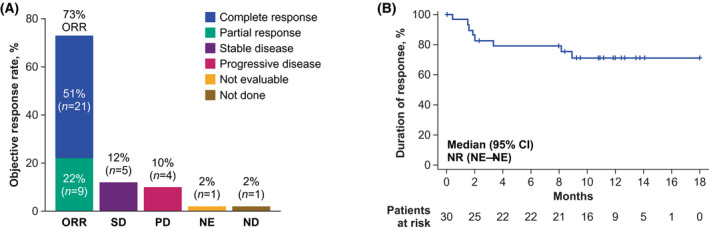
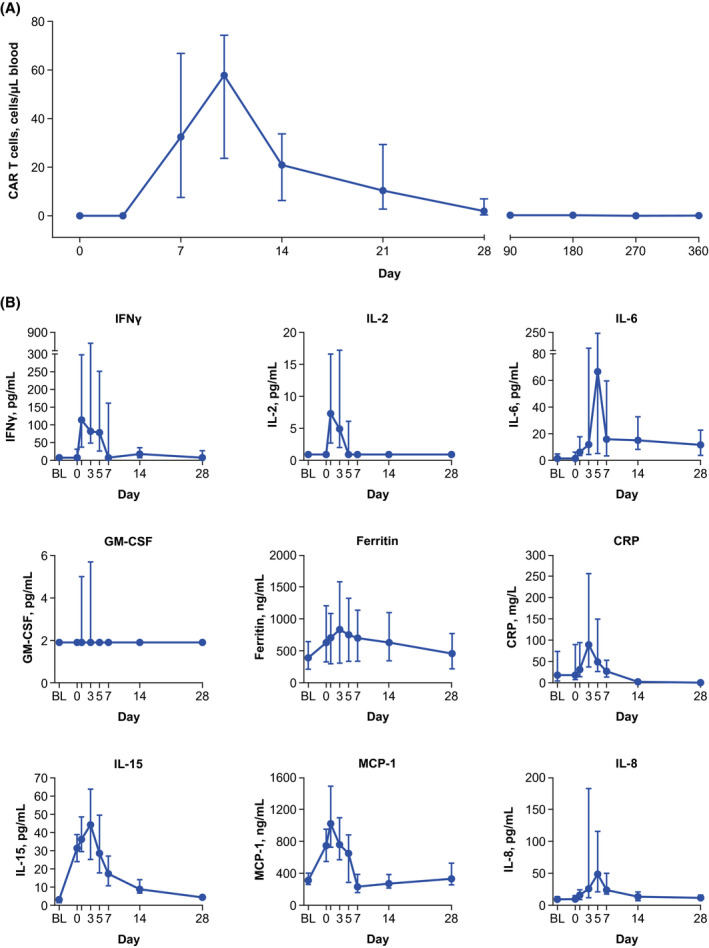
Axicabtagene ciloleucel (axi-cel) is an autologous anti-CD19 chimeric antigen receptor (CAR) T-cell therapy approved for relapsed or refractory large B-cell lymphoma (R/R LBCL). To reduce axi-cel-related toxicity, several exploratory safety management cohorts were added to ZUMA-1 (NCT02348216), the pivotal phase 1/2 study of axi-cel in refractory LBCL. Cohort 4 evaluated the rates and severity of cytokine release syndrome (CRS) and neurologic events (NEs) with earlier corticosteroid and tocilizumab use. Primary endpoints were incidence and severity of CRS and NEs. Patients received 2 × 106 anti-CD19 CAR T cells/kg after conditioning chemotherapy. Forty-one patients received axi-cel. Incidences of any-grade CRS and NEs were 93% and 61%, respectively (grade ≥ 3, 2% and 17%). There was no grade 4 or 5 CRS or NE. Despite earlier dosing, the cumulative cortisone-equivalent corticosteroid dose in patients requiring corticosteroid therapy was lower than that reported in the pivotal ZUMA-1 cohorts. With a median follow-up of 14·8 months, objective and complete response rates were 73% and 51%, respectively, and 51% of treated patients were in ongoing response. Earlier and measured use of corticosteroids and/or tocilizumab has the potential to reduce the incidence of grade ≥ 3 CRS and NEs in patients with R/R LBCL receiving axi-cel.
Keywords: CAR T; axi-cel; corticosteroids; large B-cell lymphoma; toxicity.
© 2021 The Authors. British Journal of Haematology published by British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
MST has served in a consultancy or advisory role for Amgen, Kite, a Gilead Company, Celgene, Regeneron and Roche, and received research funding from Amgen, Kite, a Gilead Company, Regeneron, Roche and MacroGenics. TvM has received honoraria from Kite, a Gilead Company, and has served in a consultant or advisory role for Janssen. RH has received honoraria from Bristol Myers Squibb, Novartis, Celgene, Janssen, MSD, Kite, a Gilead Company, Roche, and ADC Therapeutics and has served in a consultancy or advisory role for Kite, a Gilead Company. MCM has served in a consultancy or advisory role for Janssen‐Cilag, Gilead, and Alnylam and has received travel support from Celgene. KB has served in a consultancy or advisory role for Kite, a Gilead Company, Roche, Sandoz, and Takeda; received honoraria from Kite, a Gilead Company, Celgene, Roche and Takeda; and received travel support from Roche. PJL has served in a consultancy or advisory role for Takeda, Servier, Roche, Bristol Myers Squibb, Celgene, Sandoz, and Genmab and received research funding from Takeda and Servier. CT has served in a consultancy or advisory role for Novartis, Roche, Celgene, and Janssen; received honoraria from Gilead, Novartis, Roche, Celgene and Janssen; received research funding from Roche; and received travel support from Gilead, Novartis, Roche and Janssen. MW has served in a consultancy or advisory role for Kite, a Gilead Company, Novartis, Bristol Myers Squibb, AstraZeneca, Pfizer, Merck, Genmab and Boehringer Ingelheim; received honoraria from Novartis, Bristol Myers Squibb, AstraZeneca, Pfizer and Merck; and received travel support from Novartis, Bristol Myers Squibb and AstraZeneca. KWS has received honoraria from and has served in a consultancy or advisory role for Kite, a Gilead Company. JK has served in a consultancy or advisory role for AbbVie, Bristol Myers Squibb, Gilead, Karyopharm, Merck, Roche and Seattle Genetics; received honoraria from Amgen, AstraZeneca, Bristol Myers Squibb, Celgene, Gilead, Janssen, Karyopharm, Merck, Novartis, Roche and Seattle Genetics; and received research funding from Roche and Janssen. UD served in a consultancy or advisory role for AbbVie, Amgen, CPT, Gilead, Janssen, Novartis and Takeda; received honoraria from AbbVie, Amgen, Celgene, CPT, Gilead, Janssen, Novartis, Roche and Takeda; received research funding from Amgen, Celgene and Roche; and received travel support from AbbVie and Janssen. YZ, MS, JJK, and AK are employed by Kite, a Gilead Company, and have stock or other ownership in Gilead Sciences. SV is employed by and has received research funding and travel support from Kite, a Gilead Company, and has stock or other ownership in Gilead Sciences. JD is employed by Kite, a Gilead Company; has served in a consultancy or advisory role for GliaCure/Tufts; and has received patents, royalties or other intellectual property from Patent US8598141 (Dec 03, 2013). AB is employed by Kite, a Gilead Company, and has stock or other ownership in, has served in a consultancy or advisory role for, and received travel support from Gilead Sciences. JMR is employed by Kite, a Gilead Company. VP is employed by and has received honoraria and travel support from Kite, a Gilead Company; has stock or other ownership in Gilead Sciences; and has patents, royalties or other intellectual property from Genentech. MJK has served in a consultancy or advisory role for and received honoraria from Kite, a Gilead Company, Novartis and Miltenyi; received research funding from Roche, Takeda and Celgene; and received travel support from Kite, a Gilead Company, Novartis and Miltenyi. The remaining author (IA) declares no competing financial interests.
Figures
Comment in
-
Early immunomodulators with CAR T-cell immunotherapy in the COVID-19 era.Lancet Oncol. 2022 Jan;23(1):16-18. doi: 10.1016/S1470-2045(21)00695-1. Lancet Oncol. 2022. PMID: 34973215 Free PMC article. No abstract available.
References
-
- YESCARTA® (axicbatagene ciloleucel) Summary of product characteristics. Kite Pharma EU B.V.; 2021.
-
- YESCARTA® (axicabtagene ciloleucel) Prescribing information. Kite Pharma, Inc; 2021.
-
- Jacobson C, Locke FL, Ghobadi A, Miklos DB, Lekakis LJ, Oluwole OO, et al. Long‐term survival and gradual recovery of B cells in patients with refractory large B cell lymphoma treated with axicabtagene ciloleucel (axi‐cel). Blood. 2020;136(Suppl 1):40–2.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
