

Comparative Effectiveness of Stereotactic Electroencephalography Versus Subdural Grids in Epilepsy Surgery
- PMID: 34590337
- PMCID: PMC9438788
- DOI: 10.1002/ana.26238
Comparative Effectiveness of Stereotactic Electroencephalography Versus Subdural Grids in Epilepsy Surgery
Abstract
Objective: The aim was to compare the outcomes of subdural electrode (SDE) implantations versus stereotactic electroencephalography (SEEG), the 2 predominant methods of intracranial electroencephalography (iEEG) performed in difficult-to-localize drug-resistant focal epilepsy.
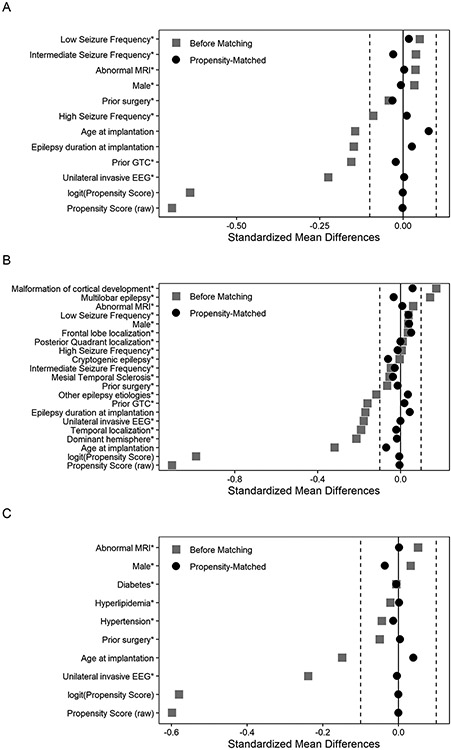
Methods: The Surgical Therapies Commission of the International League Against Epilepsy created an international registry of iEEG patients implanted between 2005 and 2019 with ≥1 year of follow-up. We used propensity score matching to control exposure selection bias and generate comparable cohorts. Study endpoints were: (1) likelihood of resection after iEEG; (2) seizure freedom at last follow-up; and (3) complications (composite of postoperative infection, symptomatic intracranial hemorrhage, or permanent neurological deficit).
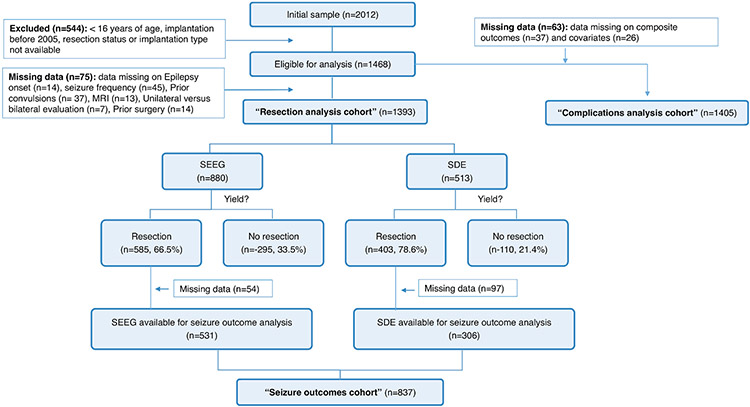
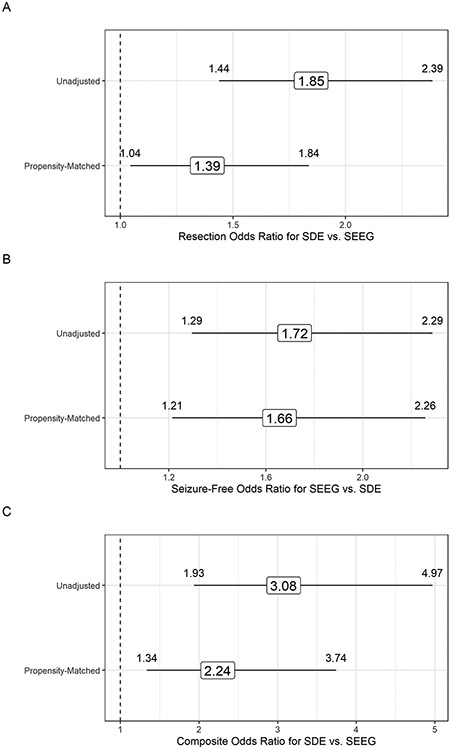
Results: Ten study sites from 7 countries and 3 continents contributed 2,012 patients, including 1,468 (73%) eligible for analysis (526 SDE and 942 SEEG), of whom 988 (67%) underwent subsequent resection. Propensity score matching improved covariate balance between exposure groups for all analyses. Propensity-matched patients who underwent SDE had higher odds of subsequent resective surgery (odds ratio [OR] = 1.4, 95% confidence interval [CI] 1.05, 1.84) and higher odds of complications (OR = 2.24, 95% CI 1.34, 3.74; unadjusted: 9.6% after SDE vs 3.3% after SEEG). Odds of seizure freedom in propensity-matched resected patients were 1.66 times higher (95% CI 1.21, 2.26) for SEEG compared with SDE (unadjusted: 55% seizure free after SEEG-guided resections vs 41% after SDE).
Interpretation: In comparison to SEEG, SDE evaluations are more likely to lead to brain surgery in patients with drug-resistant epilepsy but have more surgical complications and lower probability of seizure freedom. This comparative-effectiveness study provides the highest feasible evidence level to guide decisions on iEEG. ANN NEUROL 2021;90:927-939.
© 2021 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
None
Figures
References
-
- Jayakar P, Gotman J, Harvey AS, et al. Diagnostic utility of invasive EEG for epilepsy surgery: Indications, modalities, and techniques. Epilepsia. 2016. Nov;57(11):1735–47. - PubMed
-
- Kim LH, Parker JJ, Ho AL, et al. Postoperative outcomes following pediatric intracranial electrode monitoring: A case for stereoelectroencephalography (SEEG). Epilepsy Behav. 2020. Mar;104(Pt A):106905. - PubMed
-
- Joswig H, Lau JC, Abdallat M, et al. Stereoelectroencephalography Versus Subdural Strip Electrode Implantations: Feasibility, Complications, and Outcomes in 500 Intracranial Monitoring Cases for Drug-Resistant Epilepsy. Neurosurgery. 2020. Jul 1;87(1):E23–e30. - PubMed
