

Burden of invasive group B Streptococcus disease in non-pregnant adults: A systematic review and meta-analysis
- PMID: 34591924
- PMCID: PMC8483371
- DOI: 10.1371/journal.pone.0258030
Burden of invasive group B Streptococcus disease in non-pregnant adults: A systematic review and meta-analysis
Abstract
Background: Streptococcus agalactiae or group B Streptococcus (GBS) has emerged as an important cause of invasive disease in adults, particularly among the elderly and those with underlying comorbidities. Traditionally, it was recognised as an opportunistic pathogen colonising and causing disease in pregnant women, neonates, and young infants. Reasons for the upsurge of invasive GBS (iGBS) among the elderly remain unclear, although it has been related to risk factors such as underlying chronic diseases, immunosenescence, impaired inflammatory response, and spread of virulent clones. Antibiotics are successfully as treatment or prophylaxis against iGBS. Several candidate vaccines against iGBS are under development.
Objectives: To conduct a systematic review of the current literature on invasive GBS in order to determine disease incidence and case fatality ratio (CFR) among non-pregnant adults. Additionally, information on risk factors, clinical presentation, serotype distribution, and antimicrobial resistance was also retrieved.
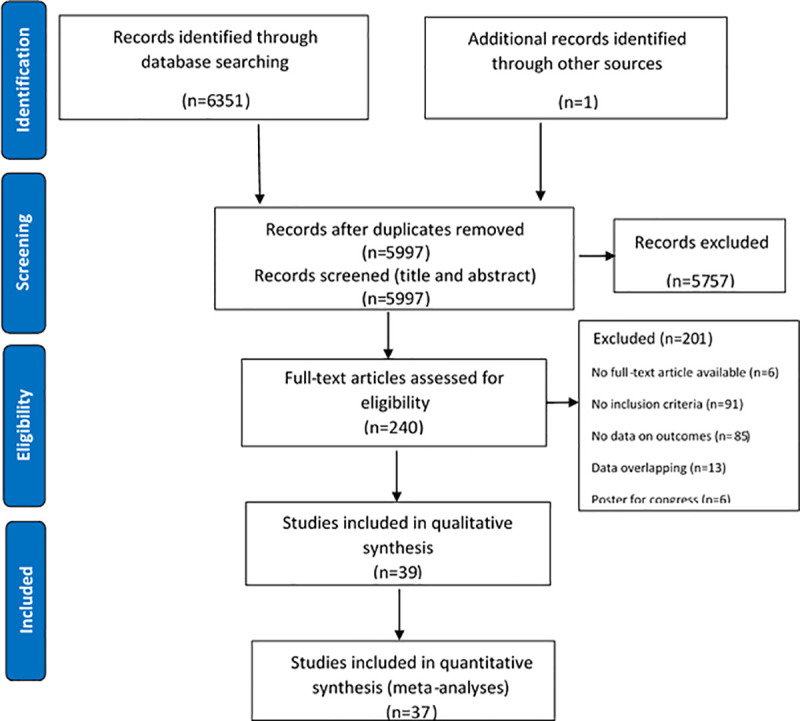
Methods: Between January and June 2020, electronic searches were conducted in relevant databases: MEDLINE, EMBASE, Global Health, and SCOPUS. Studies were included in the systematic review if they met the inclusion/exclusion criteria. The authors assessed the selected studies for relevance, risk of bias, outcome measures, and heterogeneity. Meta-analyses on incidence and CFR were conducted after evaluating the quality of methods for assessment of exposure and outcomes.
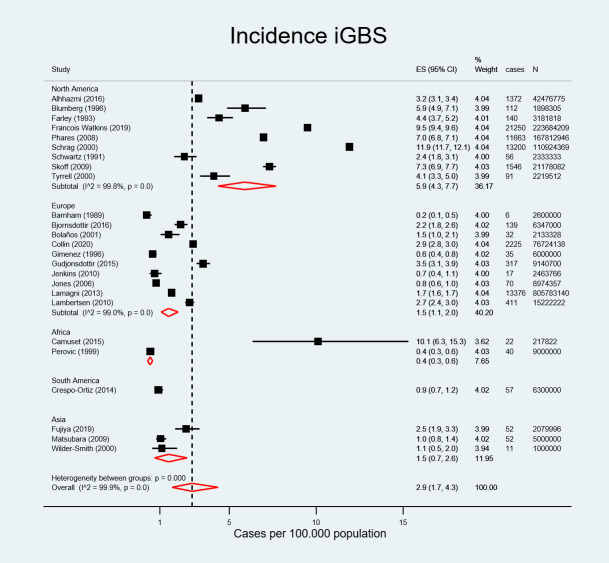
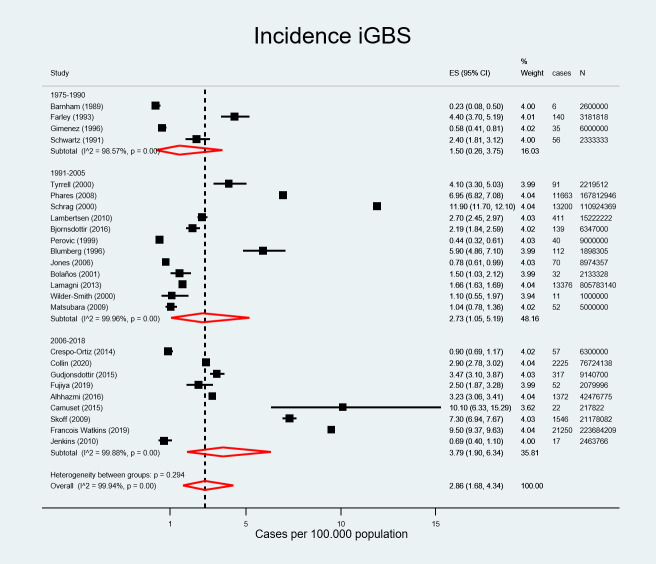
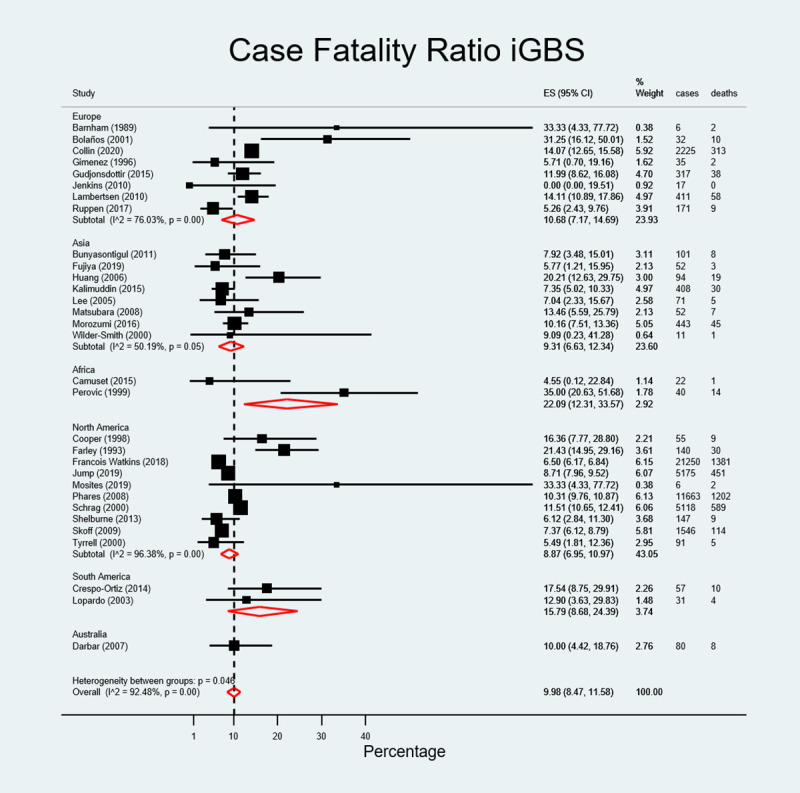
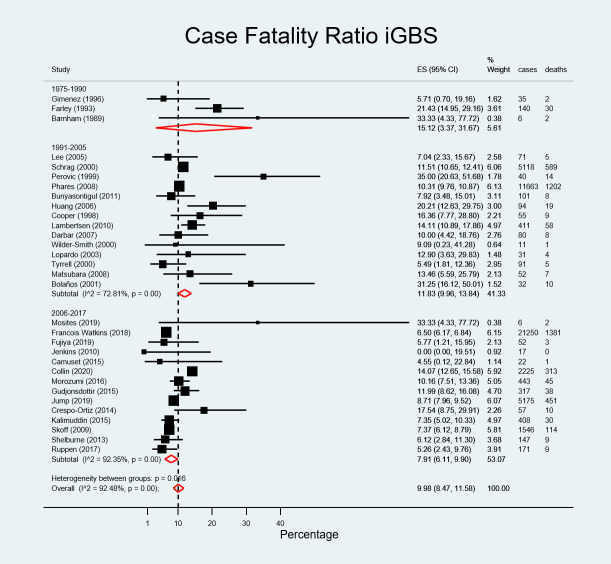
Results: Pooled estimates of iGBS incidence in non-pregnant adults 15 years and older were 2.86 cases per 100.000 population (95% CI, 1.68-4.34). Incidence rates in older adults were substantially higher, 9.13 (95%CI, 3.53-17.22) and 19.40 (95%CI, 16.26-22.81) per 100.000 population ≥50 and ≥ 65 years old, respectively. Incidence rates ranged from 0.40 (95% CI, 0.30-0.60) in Africa to 5.90 cases per 100.000 population (95% CI, 4.30-7.70) in North America. The overall CFR was and 9.98% (95% CI, 8.47-11.58). CFR was highest in Africa at 22.09% (95% CI, 12.31-33.57). Serotype V was the most prevalent serotype globally and in North America accounting for 43.48% (n = 12926) and 46,72% (n = 12184) of cases, respectively. Serotype Ia was the second and serotype III was more prevalent in Europe (25.0%) and Asia (29.5%). Comorbidities were frequent among non-pregnant adult iGBS cases. Antimicrobial resistance against different antibiotics (i.e., penicillin, erythromycin) is increasing over time.
Conclusions: This systematic review revealed that iGBS in non-pregnant adults has risen in the last few years and has become a serious public health threat especially in older adults with underlying conditions. Given the current serotype distribution, vaccines including serotypes predominant among non-pregnant adults (i.e., serotypes V, Ia, II, and III) in their formulation are needed to provide breadth of protection. Continued surveillance monitoring potential changes in serotype distribution and antimicrobial resistance patterns are warranted to inform public health interventions.
Conflict of interest statement
All authors are employees of Pfizer and may hold stock options. Pfizer supported the work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
