

Cost-effectiveness of Venous Thromboembolism Prophylaxis After Hospitalization in Patients With Inflammatory Bowel Disease
- PMID: 34591970
- PMCID: PMC9890631
- DOI: 10.1093/ibd/izab246
Cost-effectiveness of Venous Thromboembolism Prophylaxis After Hospitalization in Patients With Inflammatory Bowel Disease
Abstract
Background: Patients with inflammatory bowel disease (IBD) have a 2- to 3-fold greater risk of venous thromboembolism (VTE) than patients without IBD, with increased risk during hospitalization that persists postdischarge. We determined the cost-effectiveness of postdischarge VTE prophylaxis among hospitalized patients with IBD.
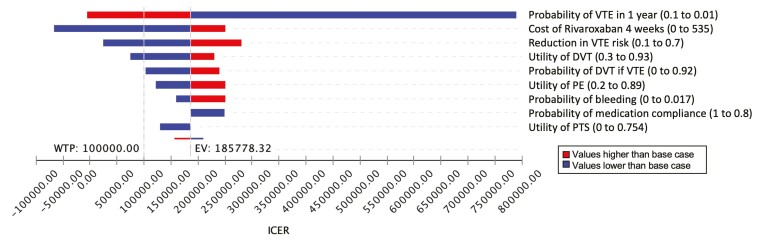
Methods: A decision tree compared inpatient prophylaxis alone vs 4 weeks of postdischarge VTE prophylaxis with 10 mg/day of rivaroxaban. Our primary outcome was quality-adjusted life years (QALYs) over 1 year, and strategies were compared using a willingness to pay of $100,000/QALY from a societal perspective. Costs (in 2020 $USD), incremental cost-effectiveness ratios (ICERs) and number needed to treat (NNT) to prevent 1 VTE and VTE death were calculated. Deterministic 1-way and probabilistic analyses assessed model uncertainty.
Results: Prophylaxis with rivaroxaban resulted in 1.68-higher QALYs per 1000 persons compared with no postdischarge prophylaxis at an incremental cost of $185,778 per QALY. The NNT to prevent a single VTE was 78, whereas the NNT to prevent a single VTE-related death was 3190. One-way sensitivity analyses showed that higher VTE risk >4.5% and decreased cost of rivaroxaban ≤$280 can reduce the ICER to <$100,000/QALY. Probabilistic sensitivity analyses favored prophylaxis in 28.9% of iterations.
Conclusions: Four weeks of postdischarge VTE prophylaxis results in higher QALYs compared with inpatient prophylaxis alone and prevents 1 postdischarge VTE among 78 patients with IBD. Although postdischarge VTE prophylaxis for all patients with IBD is not cost-effective, it should be considered in a case-by-case scenario, considering VTE risk profile, costs, and patient preference.
Keywords: IBD; VTE; cost-effectiveness; prophylaxis.
© 2021 Crohn’s & Colitis Foundation. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures



References
-
- Grainge MJ, West J, Card TR. Venous thromboembolism during active disease and remission in inflammatory bowel disease: a cohort study. Lancet. 2010;375:657–663. - PubMed
-
- Murthy SK, Robertson McCurdy AB, Carrier M, McCurdy JD. Venous thromboembolic events in inflammatory bowel diseases: A review of current evidence and guidance on risk in the post-hospitalization setting. Thromb Res. 2020;194:26–32. - PubMed
-
- Centers for Disease Control. Venous thromboembolism in adult hospitalizations—United States, 2007-2009. MMWR Morb Mortal Wkly Rep. 2012;61:401–404. - PubMed
