

Significant Spirometric Transitions and Preserved Ratio Impaired Spirometry Among Ever Smokers
- PMID: 34592319
- PMCID: PMC8941606
- DOI: 10.1016/j.chest.2021.09.021
Significant Spirometric Transitions and Preserved Ratio Impaired Spirometry Among Ever Smokers
Abstract
Background: Emerging data from longitudinal studies suggest that preserved ratio impaired spirometry (PRISm), defined by proportionate reductions in FEV1 and FVC, is a heterogeneous population with frequent transitions to other lung function categories relative to individuals with normal and obstructive spirometry. Controversy regarding the clinical significance of these transitions exists (eg, whether transitions merely reflect measurement variability or noise).
Research question: Are individuals with PRISm enriched for transitions associated with substantial changes in lung function?
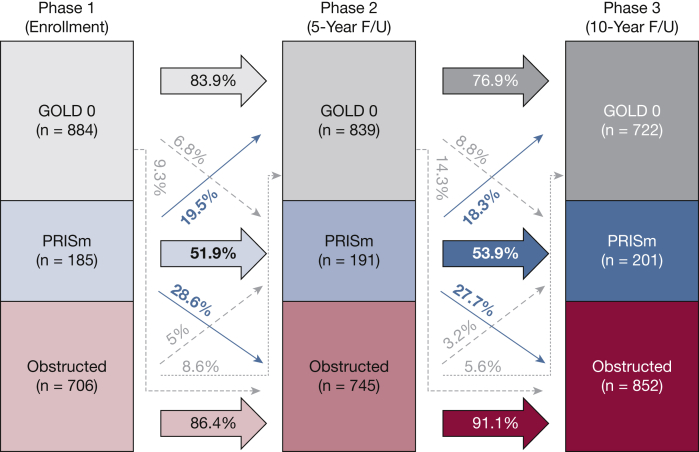
Study design and methods: Current and former smokers enrolled in the Genetic Epidemiology of COPD (COPDGene) study with spirometry available in phases 1 through 3 (enrollment, 5-year follow-up, and 10-year follow-up) were analyzed. Postbronchodilator lung function categories were as follows: PRISm (FEV1 < 80% predicted with FEV1/FVC ratio ≥ 0.7), Global Initiative for Chronic Obstructive Lung Disease grade 0 (FEV1 ≥ 80% predicted and FEV1/FVC ≥ 0.7), and obstruction (FEV1/FVC < 0.7). Significant transition status was affirmative if a subject belonged to two or more spirometric categories and had > 10% change in FEV1 % predicted and/or FVC % predicted between consecutive visits. Ever-PRISm was present if a subject had PRISm at any visit. Logistic regression examined the association between significant transitions and ever-PRISm status, adjusted for age, sex, race, FEV1 % predicted, current smoking, pack-years, BMI, and ever-positive bronchodilator response.
Results: Among subjects with complete data (N = 1,775) over 10.1 ± 0.4 years of follow-up, the prevalence of PRISm remained consistent (10.4%-11.3%) between phases 1 through 3, but nearly one-half of subjects with PRISm transitioned into or out of PRISm at each visit. Among all subjects, 19.7% had a significant transition; ever-PRISm was a significant predictor of significant transitions (unadjusted OR, 10.3; 95% CI, 7.9-13.5; adjusted OR, 14.9; 95% CI, 10.9-20.7). Results were similar with additional adjustment for radiographic emphysema and gas trapping, when lower limit of normal criteria were used to define lung function categories, and when FEV1 alone (regardless of change in FVC % predicted) was used to define significant transitions.
Interpretation: PRISm is an unstable group, with frequent significant transitions to both obstruction and normal spirometry over time.
Clinical trial registration: ClinicalTrials.gov; No.: NCT000608764; URL: www.
Clinicaltrials: gov.
Trial registration: ClinicalTrials.gov NCT00608764.
Keywords: COPD; epidemiology; lung function; restrictive spirometry.
Published by Elsevier Inc.
Figures
Comment in
-
Spirometry: The Indefinite Search for Gold.Chest. 2022 Mar;161(3):593-594. doi: 10.1016/j.chest.2022.01.004. Chest. 2022. PMID: 35256075 No abstract available.
References
-
- Backman H., Eriksson B., Hedman L., et al. Restrictive spirometric pattern in the general adult population: methods of defining the condition and consequences on prevalence. Respir Med. 2016;120:116–123. - PubMed
-
- Mannino D.M., McBurnie M.A., Tan W., et al. Restricted spirometry in the Burden of Lung Disease Study. Int J Tuberc Lung Dis. 2012;16(10):1405–1411. - PubMed
