

Troponin-Guided Coronary Computed Tomographic Angiography After Exclusion of Myocardial Infarction
- PMID: 34593122
- PMCID: PMC8482793
- DOI: 10.1016/j.jacc.2021.07.055
Troponin-Guided Coronary Computed Tomographic Angiography After Exclusion of Myocardial Infarction
Abstract
Background: Patients with suspected acute coronary syndrome in whom myocardial infarction has been excluded are at risk of future adverse cardiac events.
Objectives: This study evaluated the usefulness of high-sensitivity cardiac troponin I (hs-cTnI) to select patients for further investigation after myocardial infarction has been excluded.
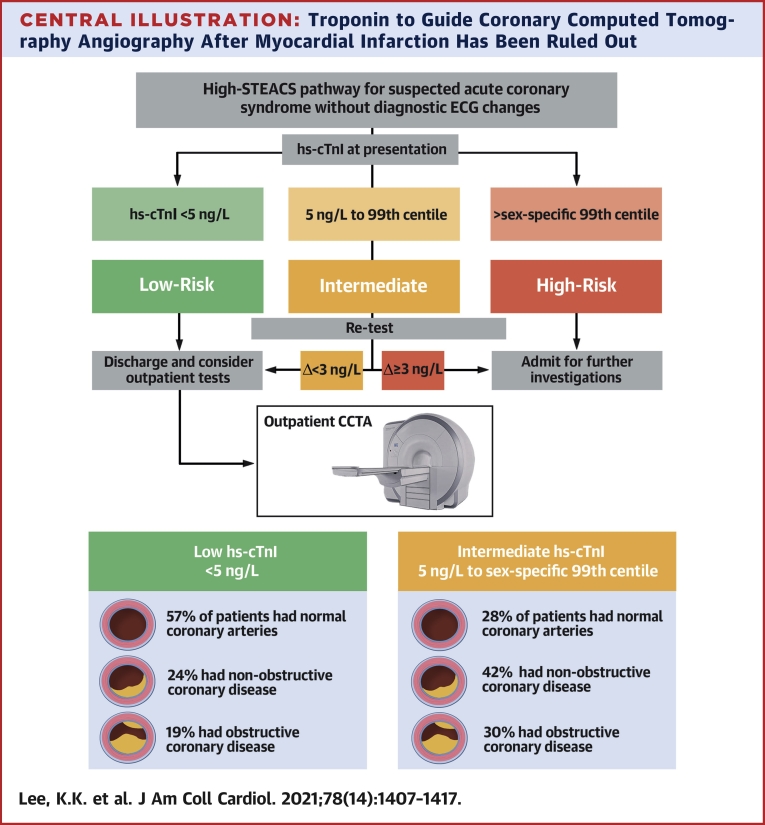
Methods: This is a prospective cohort study of patients presenting to the emergency department with suspected acute coronary syndrome and hs-cTnI concentrations below the sex-specific 99th percentile. Patients were recruited in a 2:1 fashion, stratified by peak hs-cTnI concentration above and below the risk stratification threshold of 5 ng/L. All patients underwent coronary computed tomography angiography (CCTA) after hospital discharge.
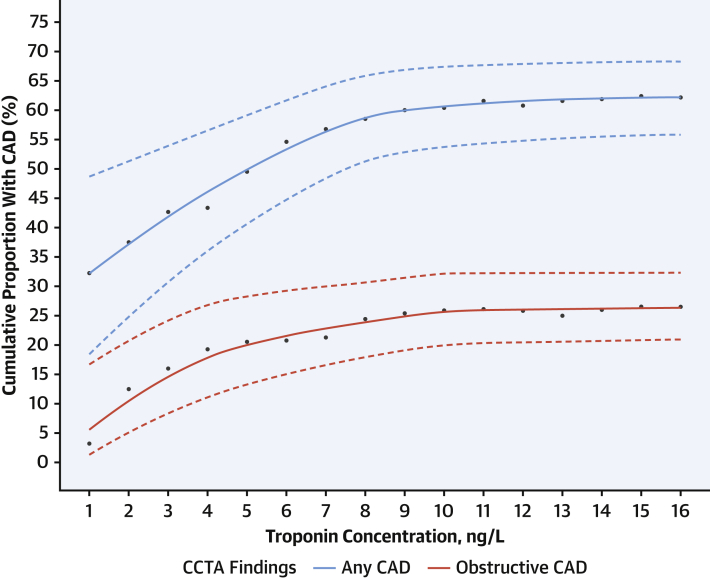
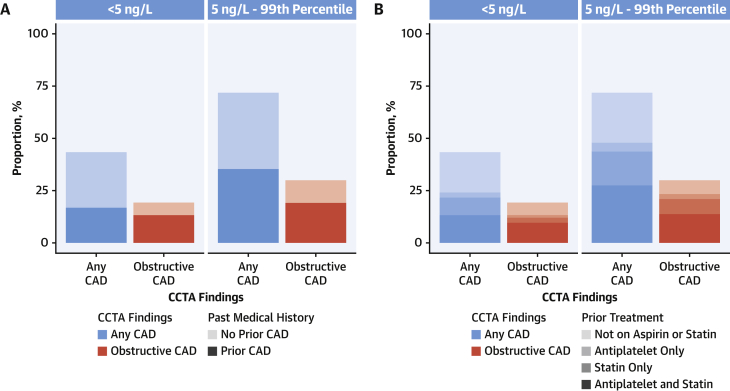
Results: Overall, 250 patients were recruited (61.4 ± 12.2 years 31% women) in whom 62.4% (156 of 250 patients) had coronary artery disease (CAD). Patients with intermediate hs-cTnI concentrations (between 5 ng/L and the sex-specific 99th percentile) were more likely to have CAD than those with hs-cTnI concentrations <5 ng/L (71.9% [120 of 167 patients] vs 43.4% [36 of 83 patients]; odds ratio: 3.33; 95% CI: 1.92-5.78). Conversely, there was no association between anginal symptoms and CAD (63.2% [67 of 106 patients] vs 61.8% [89 of 144 patients]; odds ratio: 0.92; 95% CI: 0.48-1.76). Most patients with CAD did not have a previous diagnosis (53.2%; 83 of 156 patients) and were not on antiplatelet and statin therapies (63.5%; 99 of 156 patients) before they underwent CCTA.
Conclusions: In patients who had myocardial infarction excluded, CAD was 3× more likely in those with intermediate hs-cTnI concentrations compared with low hs-cTnI concentrations. In such patients, CCTA could help to identify those with occult CAD and to target preventative treatments, thereby improving clinical outcomes.
Keywords: acute coronary syndrome; coronary computed tomography angiogram; troponin.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Lee was supported by a British Heart Foundation (BHF) Clinical Research Training Fellowship (FS/18/25/33454). Drs Bularga and Wereski and Mr. Doudesis were supported by the Medical Research Council (MR/N013166/1, MR/V007017/1, MR/V007254/1). Dr Williams was supported by the British Heart Foundation (FS/ICRF/20/26002). Dr van Beek was supported by the Scottish Imaging Network. Dr Mills was supported by a Chair Award (CH/F/21/90010), Programme Grant (RG/20/10/34966), and Research Excellence Award (RE/18/5/34216) from the British Heart Foundation. Dr Lee has received honoraria from Abbott Diagnostics. Dr van Beek is founder/owner of QCTIS Ltd; has received honoraria from Aidence NV, Roche Diagnostics, AstraZeneca, and Mentholatum; and has received research support from Siemens Healthineers. Dr Mills has received honoraria from Abbott Diagnostics, Siemens Healthineers, Roche Diagnostics, and LumiraDx; and the University of Edinburgh has received research grants from Abbott Diagnostics and Siemens Healthineers. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


Comment in
-
Biomarkers and Imaging in Chest Pain: The Iceberg Beneath the Waterline.J Am Coll Cardiol. 2021 Oct 5;78(14):1418-1420. doi: 10.1016/j.jacc.2021.08.004. J Am Coll Cardiol. 2021. PMID: 34593123 No abstract available.
References
-
- Collet J.P., Thiele H., Barbato E. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- FS/16/14/32023/BHF_/British Heart Foundation/United Kingdom
- MR/V007254/1/MRC_/Medical Research Council/United Kingdom
- CH/F/21/90010/BHF_/British Heart Foundation/United Kingdom
- CS/18/1/33711/BHF_/British Heart Foundation/United Kingdom
- RG/20/10/34966/BHF_/British Heart Foundation/United Kingdom
- RE/18/5/34216/BHF_/British Heart Foundation/United Kingdom
- MR/N013166/1/MRC_/Medical Research Council/United Kingdom
- MR/V007017/1/MRC_/Medical Research Council/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
- FS/RTF/21/30028/BHF_/British Heart Foundation/United Kingdom
- FS/18/25/33454/BHF_/British Heart Foundation/United Kingdom
- FS/ICRF/20/26002/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
