

Lipoprotein(a) has no major impact on calcification activity in patients with mild to moderate aortic valve stenosis
- PMID: 34593533
- PMCID: PMC8666821
- DOI: 10.1136/heartjnl-2021-319804
Lipoprotein(a) has no major impact on calcification activity in patients with mild to moderate aortic valve stenosis
Abstract
Objective: To assess whether patients with aortic valve stenosis (AS) with elevated lipoprotein(a) (Lp(a)) are characterised by increased valvular calcification activity compared with those with low Lp(a).
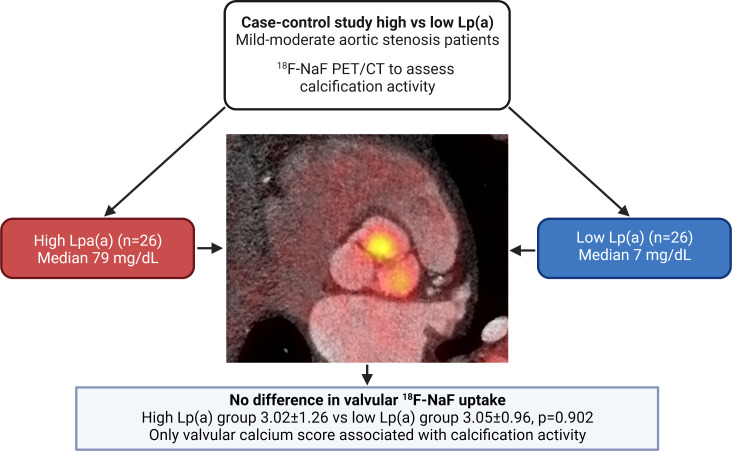
Methods: We performed 18F-sodium fluoride (18F-NaF) positron emission tomography/CT in patients with mild to moderate AS (peak aortic jet velocity between 2 and 4 m/s) and high versus low Lp(a) (>50 mg/dL vs <50 mg/dL, respectively). Subjects were matched according to age, gender, peak aortic jet velocity and valve morphology. We used a target to background ratio with the most diseased segment approach to compare 18F-NaF uptake.
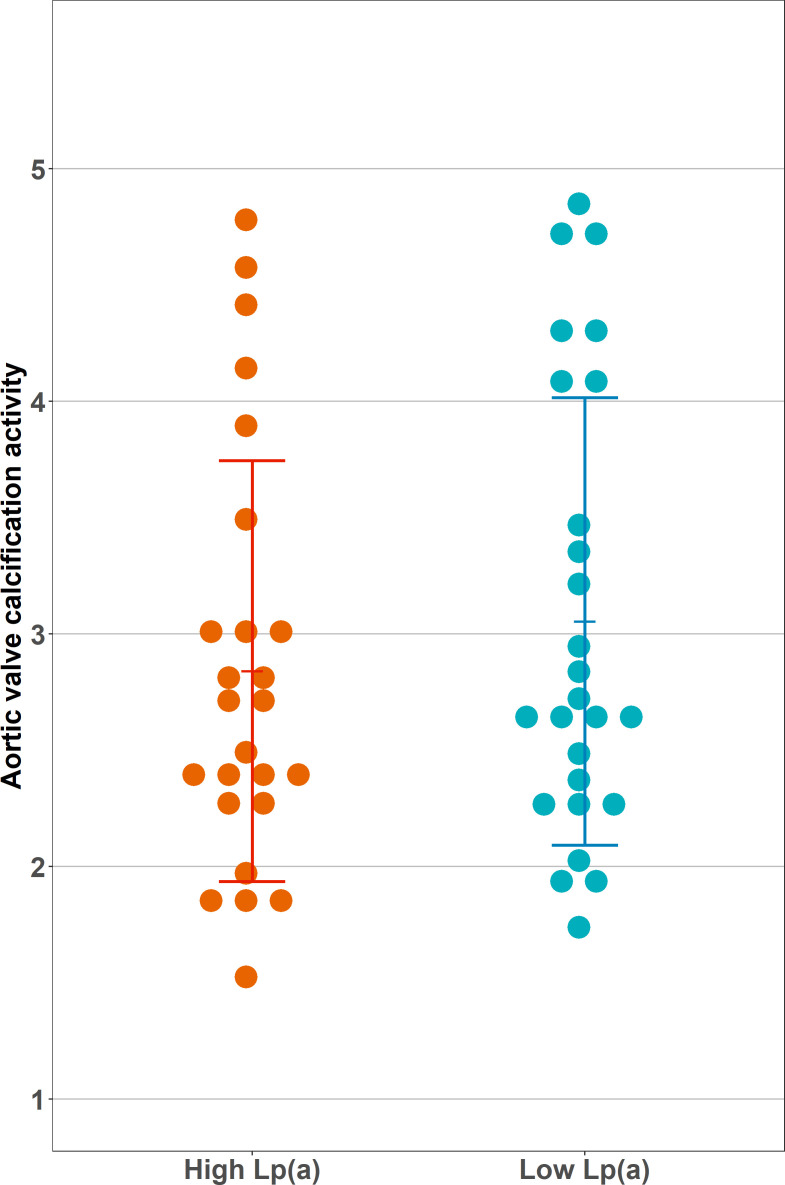
Results: 52 individuals (26 matched pairs) were included in the analysis. The mean age was 66.4±5.5 years, 44 (84.6%) were men, and the mean aortic valve velocity was 2.80±0.49 m/s. The median Lp(a) was 79 (64-117) mg/dL and 7 (5-11) mg/dL in the high and low Lp(a) groups, respectively. Systolic blood pressure and low-density-lipoprotein cholesterol (corrected for Lp(a)) were significantly higher in the low Lp(a) group (141±12 mm Hg vs 128±12 mm Hg, 2.5±1.1 mmol/L vs 1.9±0.8 mmol/L). We found no difference in valvular 18F-NaF uptake between the high and low Lp(a) groups (3.02±1.26 vs 3.05±0.96, p=0.902). Linear regression analysis showed valvular calcium score to be the only significant determinant of valvular 18F-NaF uptake (β=0.63; 95% CI 0.38 to 0.88 per 1000 Agatston unit increase, p<0.001). Lp(a) was not associated with 18F-NaF uptake (β=0.17; 95% CI -0.44 to 0.88, p=0.305 for the high Lp(a) group).
Conclusion: Among patients with mild to moderate AS, calcification activity is predominantly determined by established calcium burden. The results do not support our hypothesis that Lp(a) is associated with valvular 18F-NaF uptake.
Keywords: aortic valve stenosis; positron emission tomography computed tomography.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: ESGS has received research grants/support to his institution from Amgen, Sanofi, Resverlogix and Athera, and has served as a consultant for Amgen, Sanofi, Esperion, Novartis and Ionis Pharmaceuticals. All other authors report no conflict of interest.
Figures
Comment in
-
Lipoprotein(a) and aortic stenosis.Heart. 2022 Jan;108(1):9-10. doi: 10.1136/heartjnl-2021-320173. Epub 2021 Oct 5. Heart. 2022. PMID: 34611044 No abstract available.
-
Correspondence on "Lipoprotein(a) has no major impact on calcification activity in patients with mild to moderate aortic valve stenosis" by Kaiser et al.Heart. 2022 Apr;108(7):575-576. doi: 10.1136/heartjnl-2021-320643. Epub 2022 Jan 27. Heart. 2022. PMID: 35086886 No abstract available.
-
Response to: Correspondence on "Lipoprotein(a) has no major impact on calcification activity in patients with mild to moderate aortic valve stenosis" by Pantelidis et al.Heart. 2022 Apr;108(7):576-577. doi: 10.1136/heartjnl-2021-320644. Epub 2022 Jan 27. Heart. 2022. PMID: 35086887 No abstract available.
References
-
- Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018;392:1736–88. 10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous