

Feasibility of Acquisitions Using Total-Body PET/CT with an Ultra-Low 18F-FDG Activity
- PMID: 34593593
- PMCID: PMC9157722
- DOI: 10.2967/jnumed.121.262038
Feasibility of Acquisitions Using Total-Body PET/CT with an Ultra-Low 18F-FDG Activity
Abstract
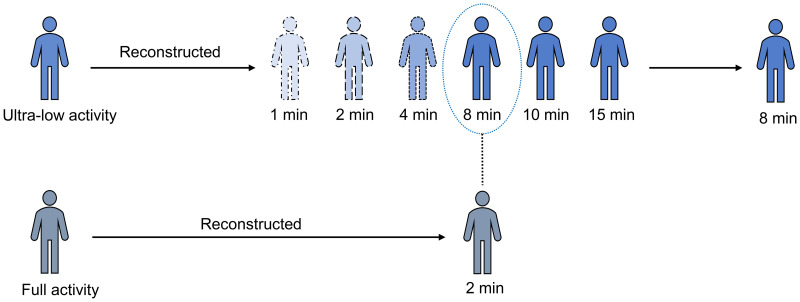
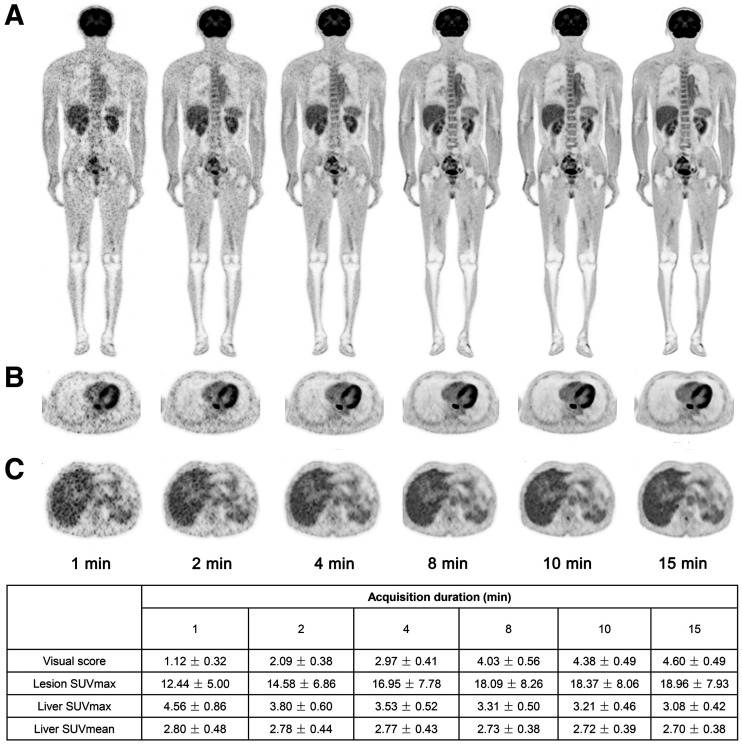
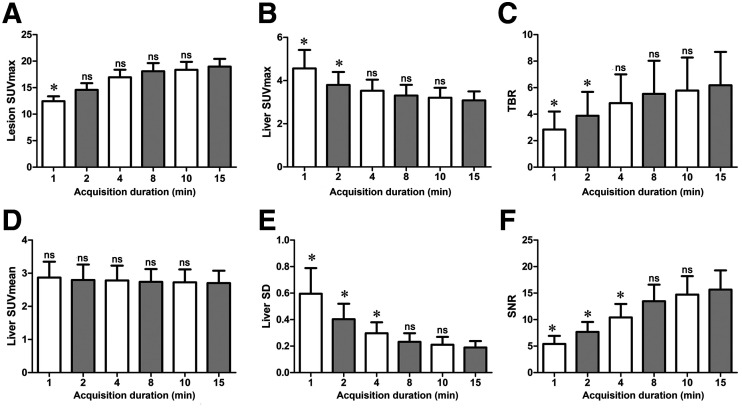
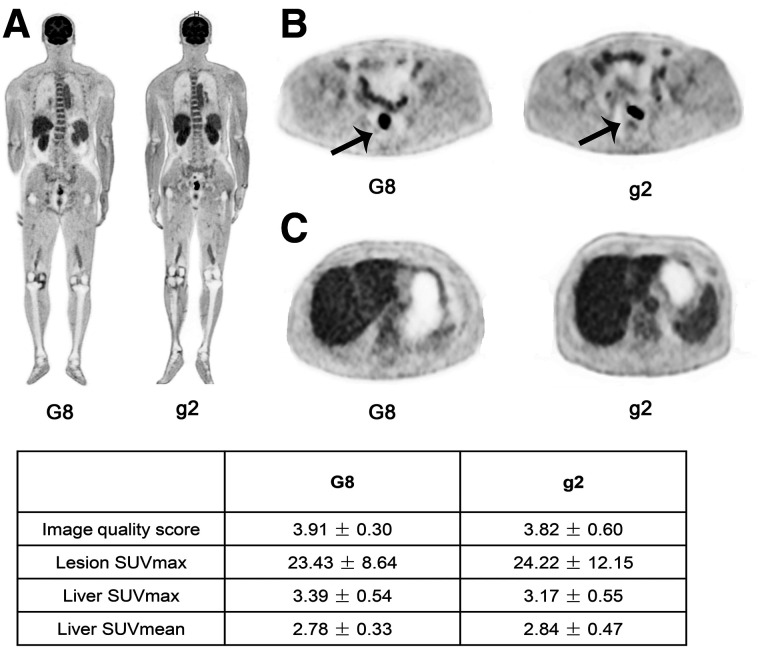
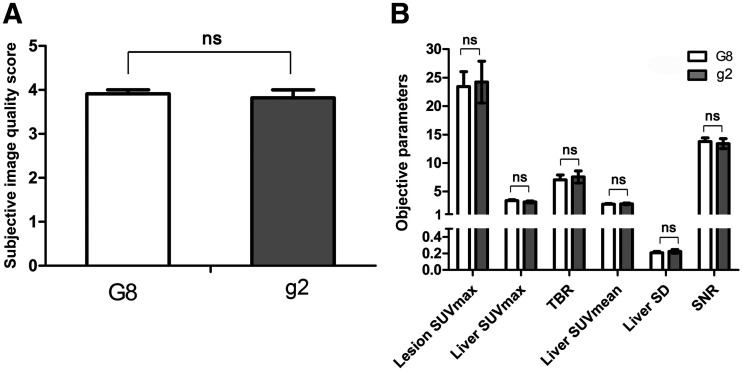
The present study aimed to evaluate the feasibility of ultra-low 18F-FDG activity in total-body PET/CT oncologic studies. Methods: Thirty patients with cancer were enrolled prospectively and underwent a total-body PET/CT scan 60 min after injection of an ultra-low 18F-FDG activity (0.37 MBq/kg). Of the 30 enrolled patients, 11 were diagnosed with colorectal cancer (CRC). PET raw data were acquired within 15 min and reconstructed using data from the first 1, 2, 4, 8, and 10 min and the entire 15 min (G1, G2, G4, G8, G10, and G15, respectively). Image quality was qualitatively assessed twice by 2 readers using a 5-point Likert scale. The Cohen κ-test was used to investigate the intra- and interreader agreement. The SUVmax of lesions; the SUVmax, SUVmean, and SD of the livers; the tumor-to-background ratio; and the signal-to-noise ratio were measured and compared. The acquisition time for a clinically acceptable image quality using an ultra-low-activity injection was determined. In a matched-pair study, 11 patients with CRC who received a full 18F-FDG activity (3.7 MBq/kg) with an acquisition time of 2 min were selected retrospectively by matching sex, height, weight, body mass index, glucose level, uptake time, and pathologic types with the 11 CRC subjects in the prospective study. Qualitative and quantitative analyses were performed and compared between the 11 patients with CRC in the ultra-low-activity group and their matched full-activity controls. Results: Qualitative analysis of image quality showed good intra- and interreader agreements (all κ > 0.7). All the images acquired for 8 min or longer scored over 3 (indicating clinical acceptability). There was no significant difference in tumor-to-background ratio and liver signal-to-noise ratio among all the images acquired for 8 min or longer. In the matched study, no significant difference was found in the image quality score and quantitative parameters between the ultra-low-activity group with an 8-min acquisition and the full-activity group with a 2-min acquisition. Conclusion: An ultra-low 18F-FDG activity with an 8-min acquisition in a total-body PET/CT study can achieve acceptable image quality equivalent to that in the full-activity group after a 2-min acquisition.
Keywords: image quality; total-body PET/CT; ultra-low activity.
© 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Martin O, Schaarschmidt BM, Kirchner J, et al. PET/MRI versus PET/CT for whole-body staging: results from a single-center observational study on 1,003 sequential examinations. J Nucl Med. 2020;61:1131–1136. - PubMed
-
- Noda Y, Goshima S, Kanematsu M, et al. 18F-FDG uptake on positron emission tomography as a predictor for lymphovascular invasion in patients with lung adenocarcinoma. Ann Nucl Med. 2016;30:11–17. - PubMed
-
- Husby JA, Reitan BC, Biermann M, et al. Metabolic tumor volume on 18F-FDG PET/CT improves preoperative identification of high-risk endometrial carcinoma patients. J Nucl Med. 2015;56:1191–1198. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical