Erector spinae plane block for spinal surgery: a systematic review and meta-analysis
- PMID: 34593667
- PMCID: PMC8494958
- DOI: 10.3344/kjp.2021.34.4.487
Erector spinae plane block for spinal surgery: a systematic review and meta-analysis
Abstract
Background: Although the erector spinae plane block has been used in various truncal surgical procedures, its clinical benefits in patients undergoing spinal surgery remain controversial. The aim of this meta-analysis was to evaluate the clinical benefits of erector spinae plane block in patients undergoing spinal surgery.
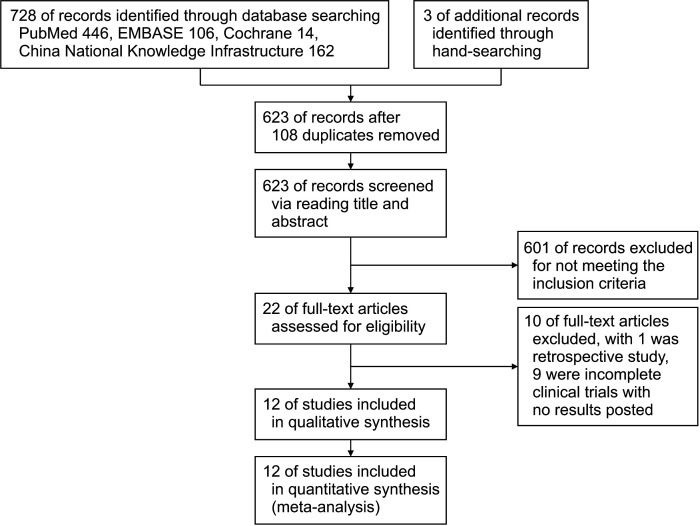
Methods: We searched the Cochrane Library, PubMed, EMBASE, and China National Knowledge Infrastructure for randomized controlled trials comparing the erector spinae plane block with a nonblocked control for spinal surgery.
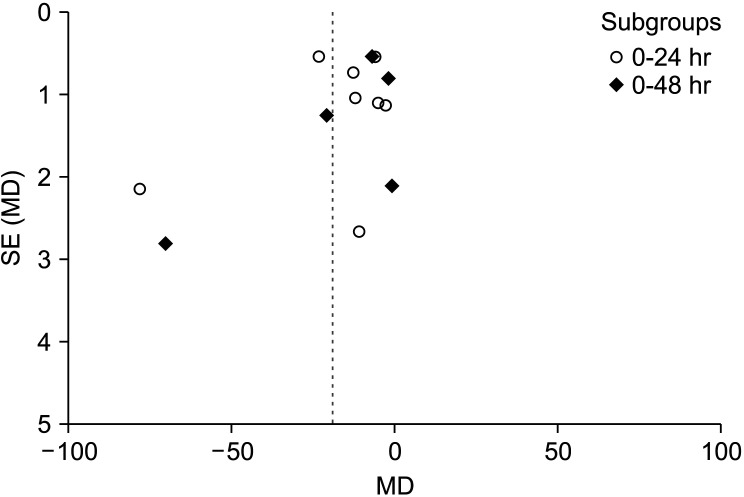
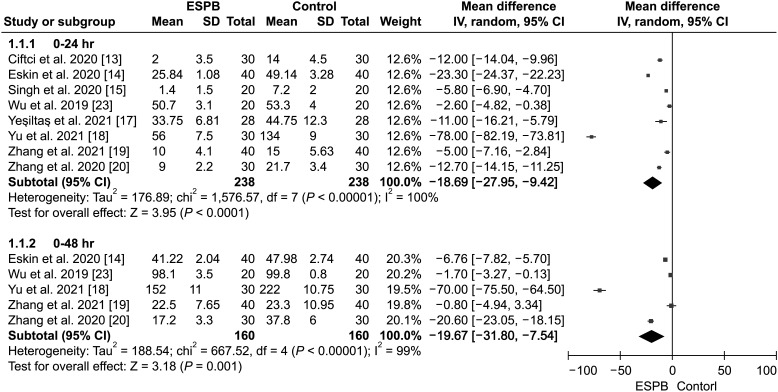
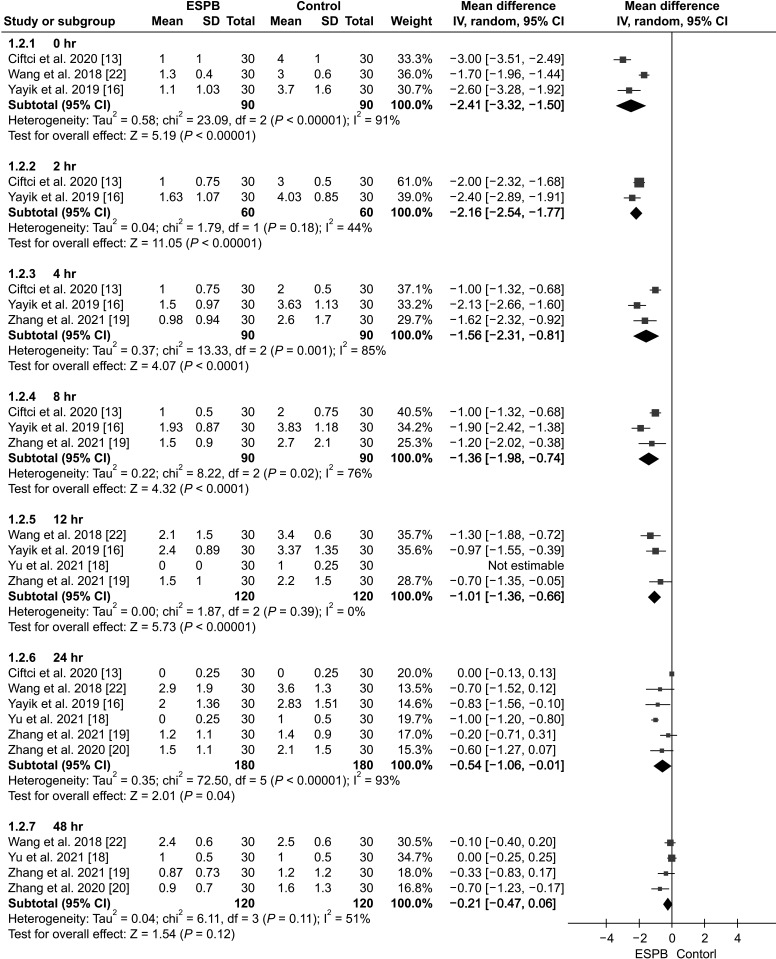
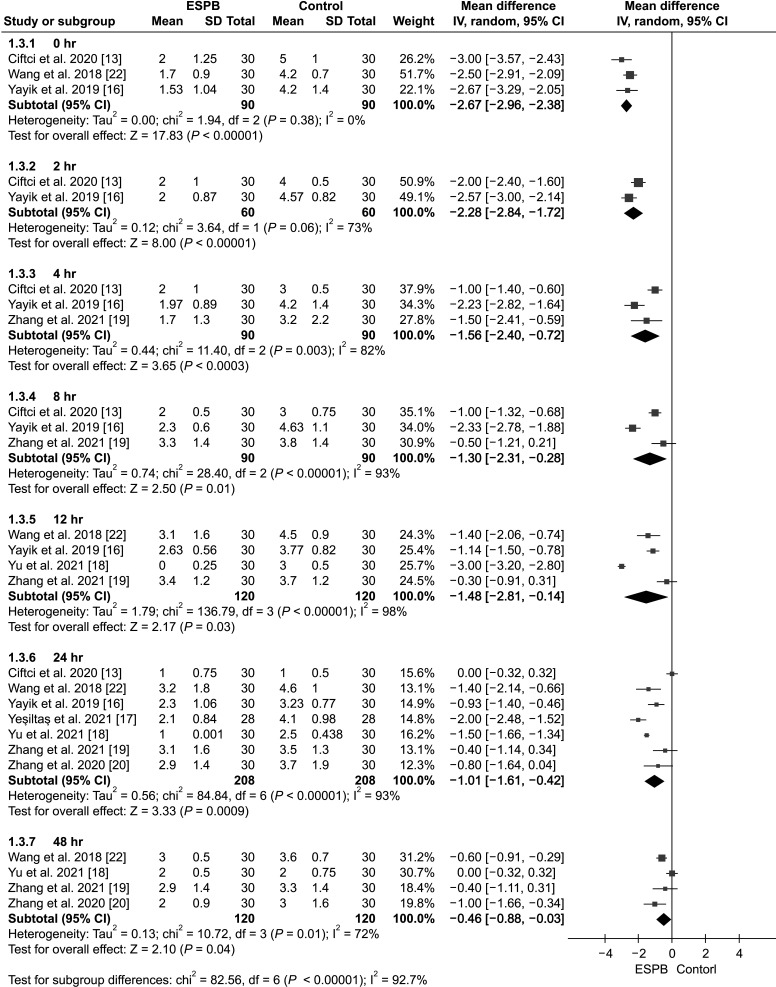
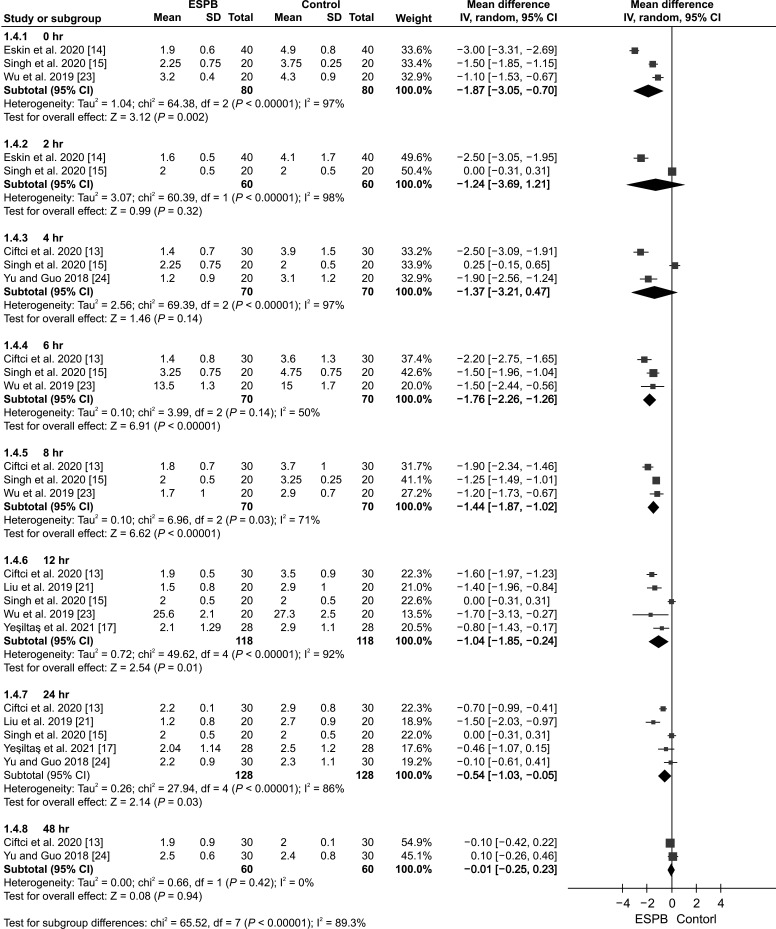
Results: Twelve studies encompassing 696 subjects were included in our systematic review and meta-analysis. We found that the erector spinae plane block decreased postoperative pain scores and opioid consumption in the postoperative and intraoperative periods. Moreover, it prolonged the time to the first rescue analgesic, reduced the number of patients who required rescue analgesia, and lowered the incidence of postoperative nausea and vomiting. However, it did not exhibit efficacy in decreasing the incidence of urinary retention and itching or shortening the length of hospital stays, or the time to first ambulation.
Conclusions: Erector spinae plane block improves analgesic efficacy among patients undergoing spinal surgery compared with nonblocked controls; however, there is insufficient evidence regarding the benefits of erector spinae plane block for rapid recovery.
Keywords: Analgesia; Analgesics; Diskectomy; Enhanced Recovery After Surgery; Erector Spinae Plane Block; Laminectomy; Meta-Analysis; Nerve Block; Neurosurgical Procedures; Opioid; Pain; Postoperative; Postoperative Nausea and Vomiting; Randomized Controlled Trial..
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Mergeay M, Verster A, Van Aken D, Vercauteren M. Regional versus general anesthesia for spine surgery. A comprehensive review. Acta Anaesthesiol Belg. 2015;66:1–9. - PubMed
LinkOut - more resources
Full Text Sources
Medical