Pharmacological and non-pharmacological strategies for preventing postherpetic neuralgia: a systematic review and network meta-analysis
- PMID: 34593669
- PMCID: PMC8494957
- DOI: 10.3344/kjp.2021.34.4.509
Pharmacological and non-pharmacological strategies for preventing postherpetic neuralgia: a systematic review and network meta-analysis
Abstract
Background: Postherpetic neuralgia (PHN) is a refractory complication of herpes zoster (HZ). To prevent PHN, various strategies have been aggressively adopted. However, the efficacy of these strategies remains controversial. Therefore, we aimed to estimate the relative efficacy of various strategies used in clinical practice for preventing PHN using a network meta-analysis (NMA).
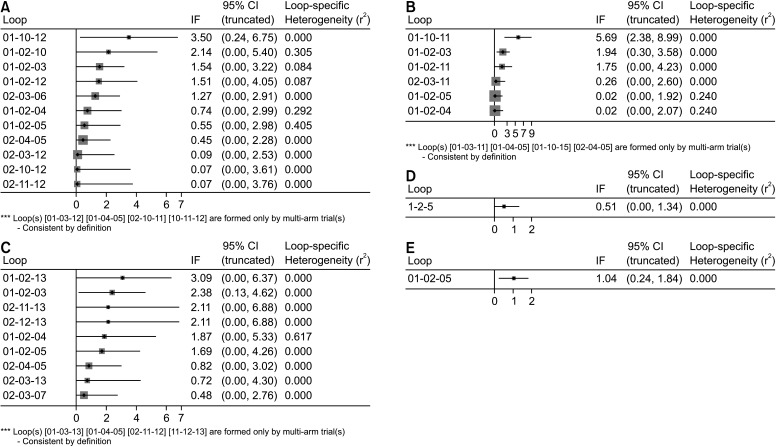
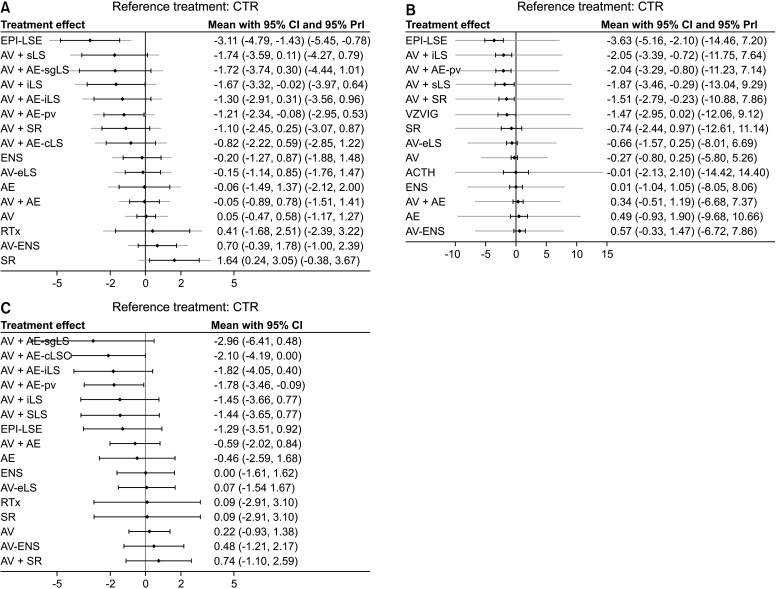
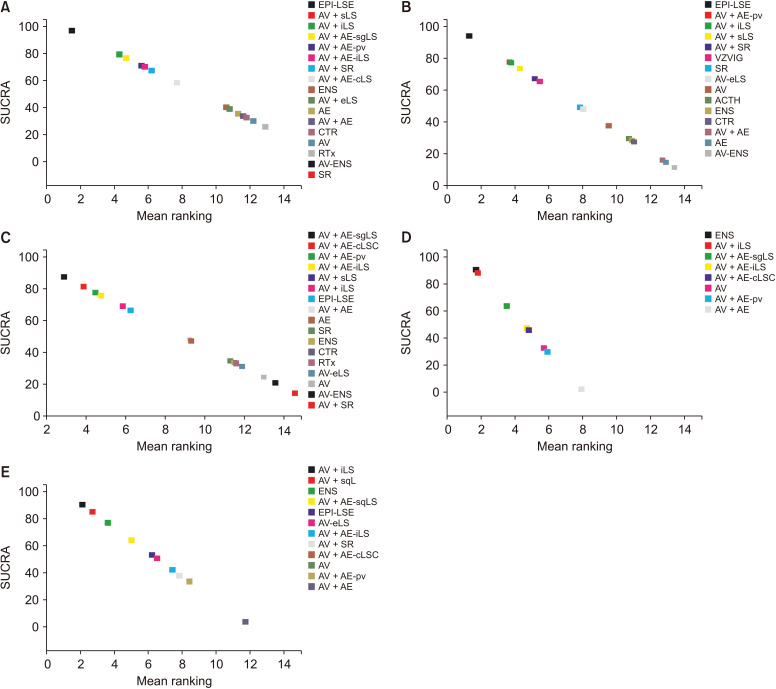
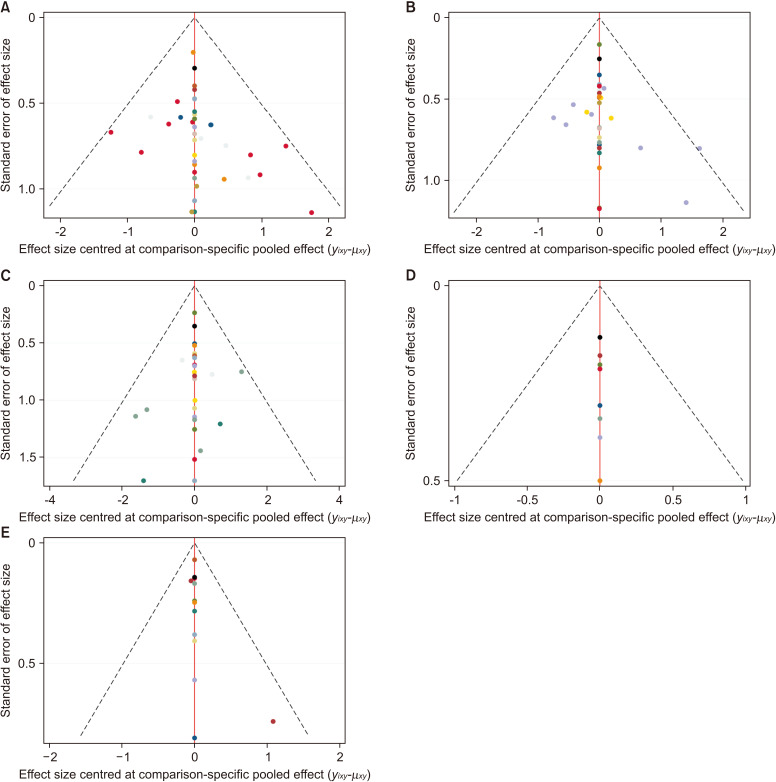
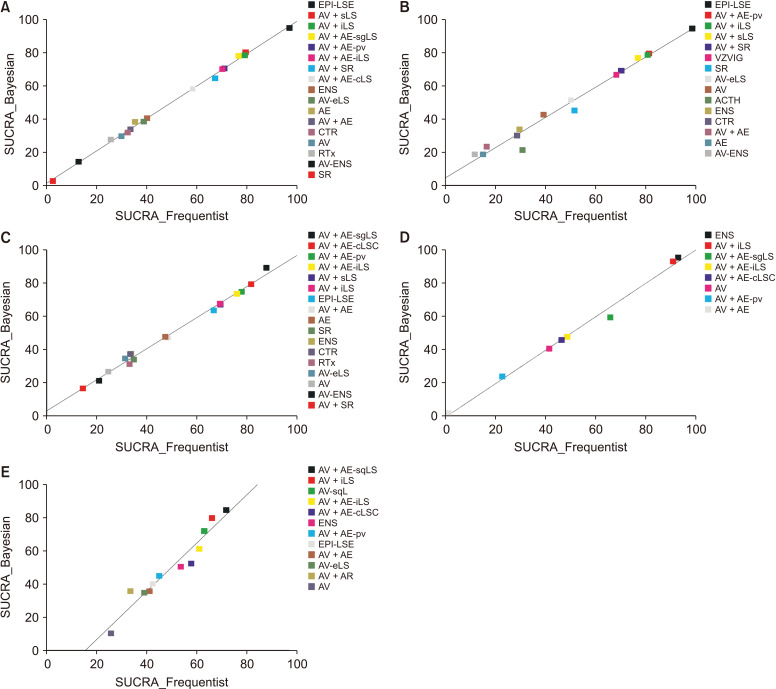
Methods: We performed a systematic and comprehensive search to identify all randomized controlled trials. The primary outcome was the incidence of PHN at 3 months after acute HZ. We performed both frequentist and Bayesian NMA and used the surface under the cumulative ranking curve (SUCRA) values to rank the interventions evaluated.
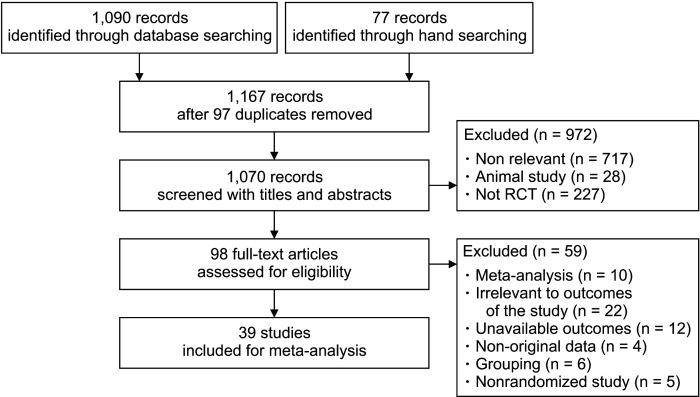
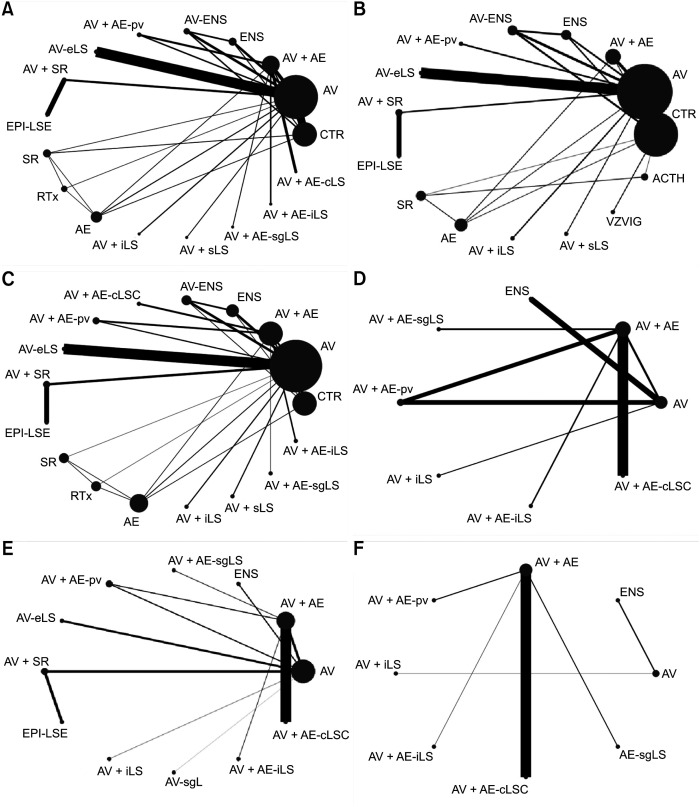
Results: In total, 39 studies were included in the systematic review and NMA. According to the SUCRA value, the incidence of PHN was lower in the order of continuous epidural block with local anesthetics and steroids (EPI-LSE), antiviral agents with subcutaneous injection of local anesthetics and steroids (AV + sLS), antiviral agents with intracutaenous injection of local anesthetics and steroids (AV + iLS) at 3 months after acute HZ. EPI-LSE, AV + sLS and AV + iLS were also effective in preventing PHN at 1 month after acute HZ. And paravertebral block combined with antiviral and antiepileptic agents was effective in preventing PHN at 1, 3, and 6 months.
Conclusions: The continuous epidural block with local anesthetics and steroid, antiviral agents with intracutaneous or subcutaneous injection of local anesthetics and a steroid, and paravertebral block combined with antiviral and antiepileptic agents are effective in preventing PHN.
Keywords: Anesthesia; Anticonvulsants; Autonomic Nerve Block; Bayes Theorem; Epidural; Injections; Local; Nerve Block; Network Meta-Analysis; Neuralgia; Postherpetic; Stellate Ganglion; Steroids; Systematic Review; Therapeutics..
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Effects of applying nerve blocks to prevent postherpetic neuralgia in patients with acute herpes zoster: a systematic review and meta-analysis.Korean J Pain. 2017 Jan;30(1):3-17. doi: 10.3344/kjp.2017.30.1.3. Epub 2016 Dec 30. Korean J Pain. 2017. PMID: 28119767 Free PMC article. Review.
-
Effect of Repetitive Intracutaneous Injections with Local Anesthetics and Steroids for Acute Thoracic Herpes Zoster and Incidence of Postherpetic Neuralgia.Pain Med. 2017 Aug 1;18(8):1566-1572. doi: 10.1093/pm/pnw190. Pain Med. 2017. PMID: 27492741 Clinical Trial.
-
Neuraxial and sympathetic blocks in herpes zoster and postherpetic neuralgia: an appraisal of current evidence.Reg Anesth Pain Med. 2004 Sep-Oct;29(5):454-61. doi: 10.1016/j.rapm.2004.04.010. Reg Anesth Pain Med. 2004. PMID: 15372391 Review.
-
Effect of Repeated Paravertebral Injections with Local Anesthetics and Steroids on Prevention of Post-herpetic Neuralgia.Pain Physician. 2020 Nov;23(6):565-572. Pain Physician. 2020. PMID: 33185373
-
The effectiveness of repetitive paravertebral injections with local anesthetics and steroids for the prevention of postherpetic neuralgia in patients with acute herpes zoster.Anesth Analg. 2009 Nov;109(5):1651-5. doi: 10.1213/ANE.0b013e3181b79075. Epub 2009 Aug 27. Anesth Analg. 2009. PMID: 19713253 Clinical Trial.
Cited by
-
Treating intractable pain with the erector spinae plane block: preventing recurrent emergency department visits and psychological distress in seniors with acute zoster pain-a case report.CJEM. 2025 Jul;27(7):568-570. doi: 10.1007/s43678-025-00924-3. Epub 2025 May 21. CJEM. 2025. PMID: 40397304 No abstract available.
-
A bibliometric analysis and visualization of acupuncture and moxibustion therapy for herpes zoster and postherpetic neuralgia.Skin Res Technol. 2024 Jun;30(6):e13815. doi: 10.1111/srt.13815. Skin Res Technol. 2024. PMID: 38924142 Free PMC article.
-
Low Trend for VZV-Associated Disease Patients to Visit Neurologists.J Multidiscip Healthc. 2023 May 16;16:1379-1392. doi: 10.2147/JMDH.S412398. eCollection 2023. J Multidiscip Healthc. 2023. PMID: 37215749 Free PMC article.
-
Correlation between pain catastrophizing in acute herpes zoster and postherpetic neuralgia: a retrospective analysis.J Anesth. 2023 Aug;37(4):589-595. doi: 10.1007/s00540-023-03208-1. Epub 2023 Jun 7. J Anesth. 2023. PMID: 37285023
-
Trigeminal Postherpetic Neuralgia: From Pathophysiology to Treatment.Curr Pain Headache Rep. 2024 Apr;28(4):295-306. doi: 10.1007/s11916-023-01209-z. Epub 2024 Jan 23. Curr Pain Headache Rep. 2024. PMID: 38261232 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources