

Immune responses to two and three doses of the BNT162b2 mRNA vaccine in adults with solid tumors
- PMID: 34594036
- PMCID: PMC9004706
- DOI: 10.1038/s41591-021-01542-z
Immune responses to two and three doses of the BNT162b2 mRNA vaccine in adults with solid tumors
Abstract
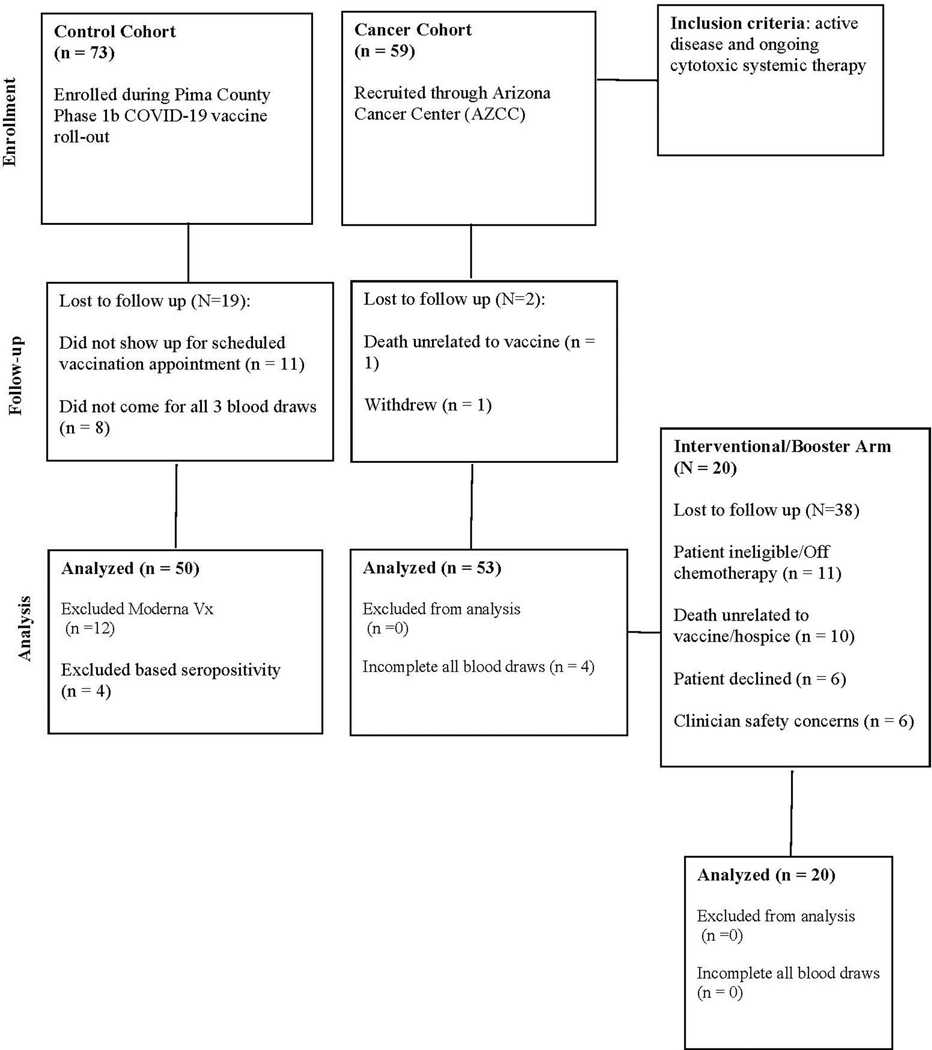
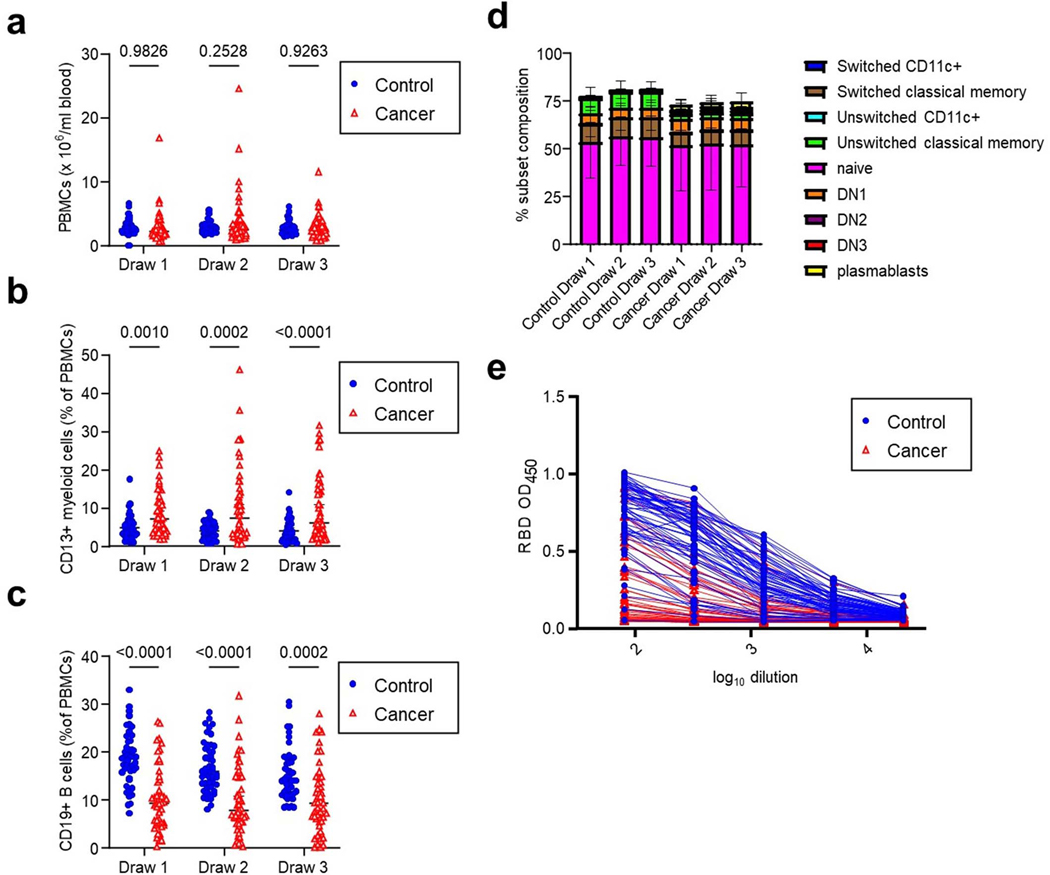
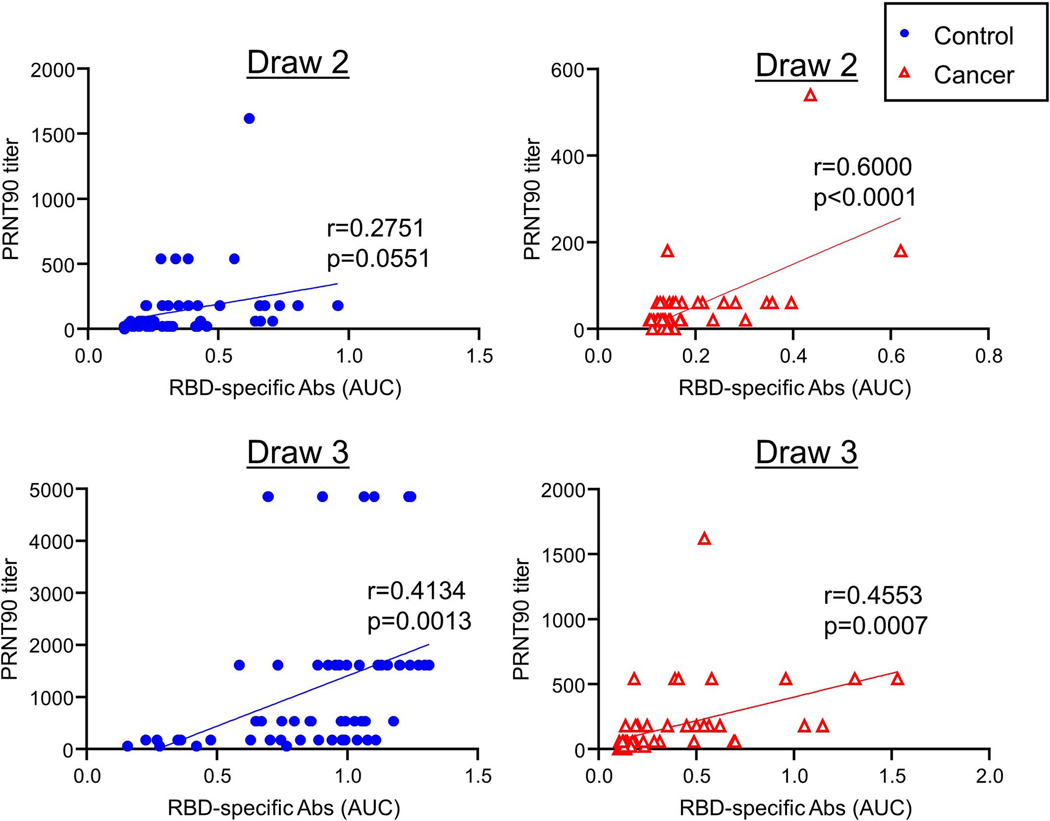
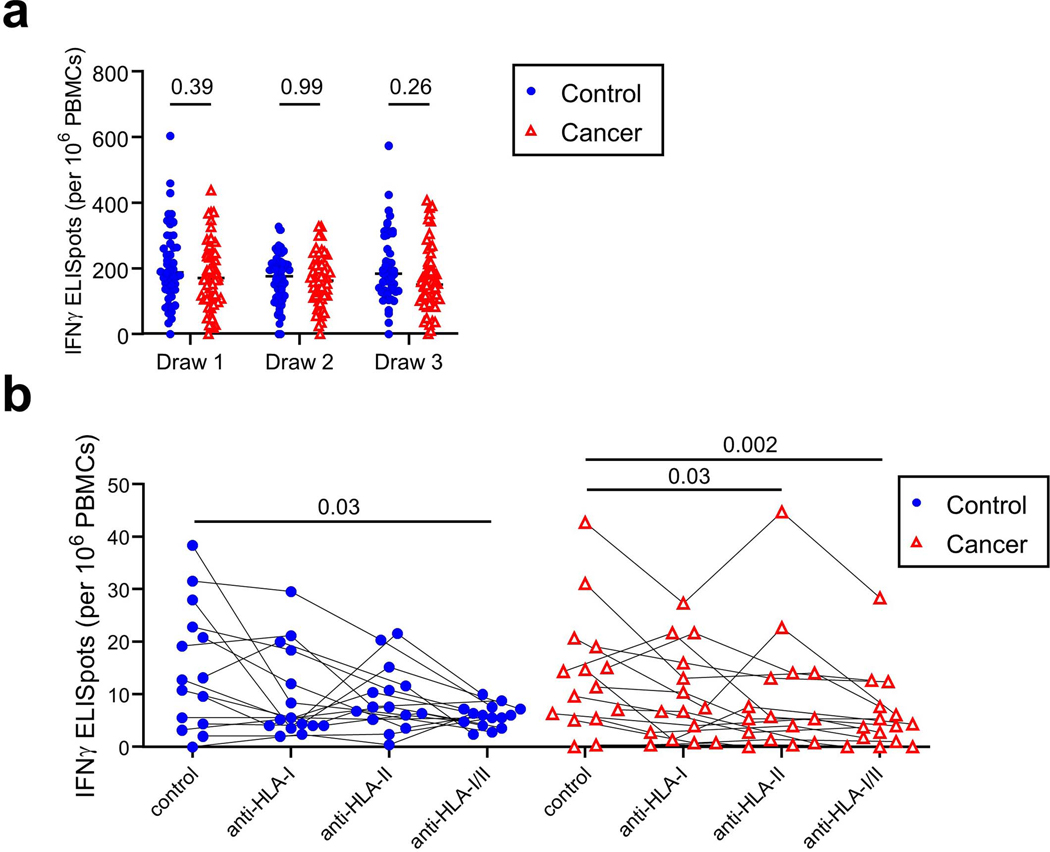
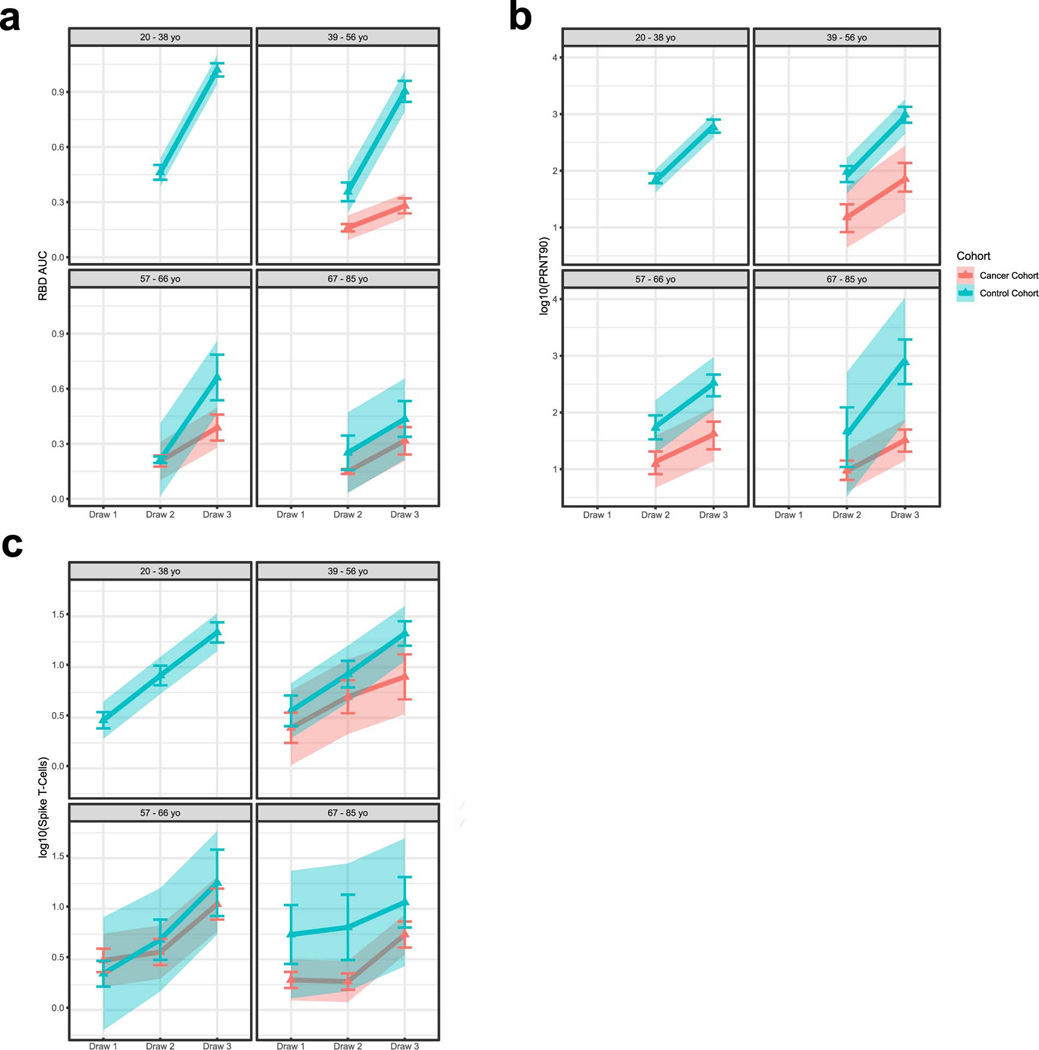
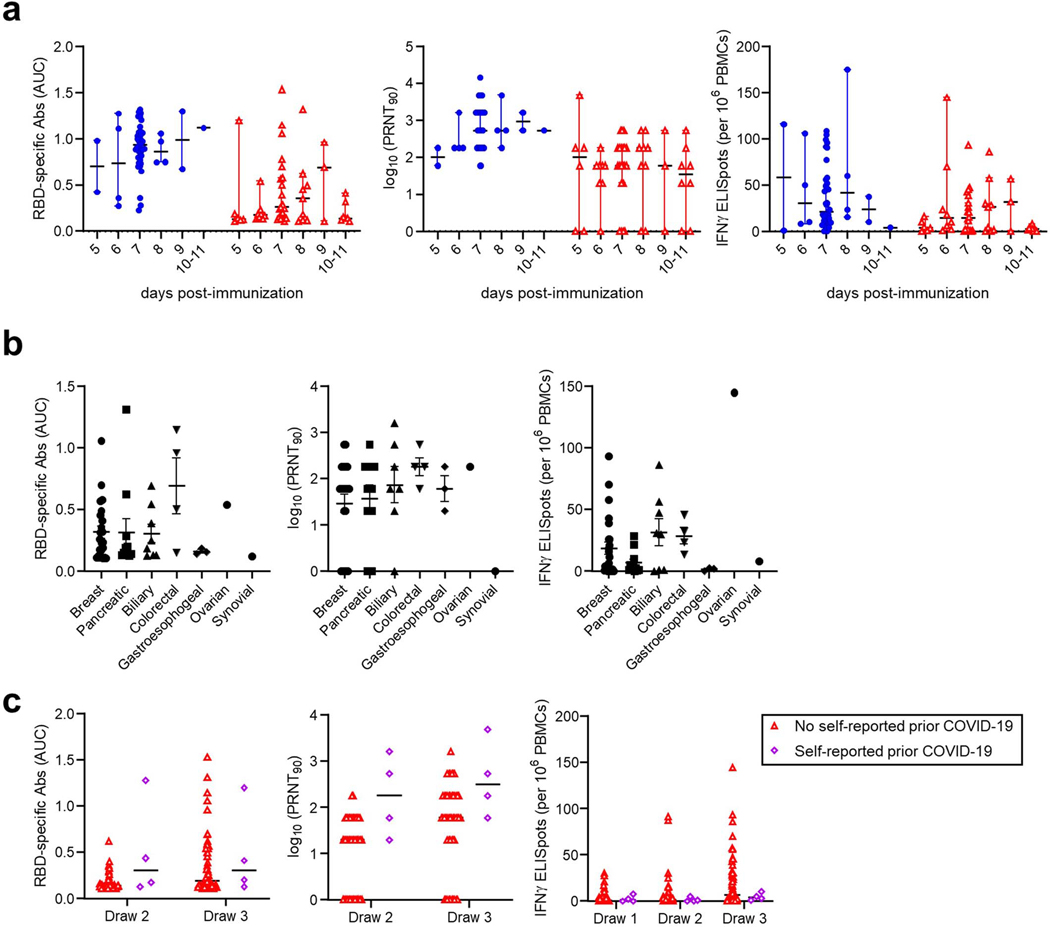
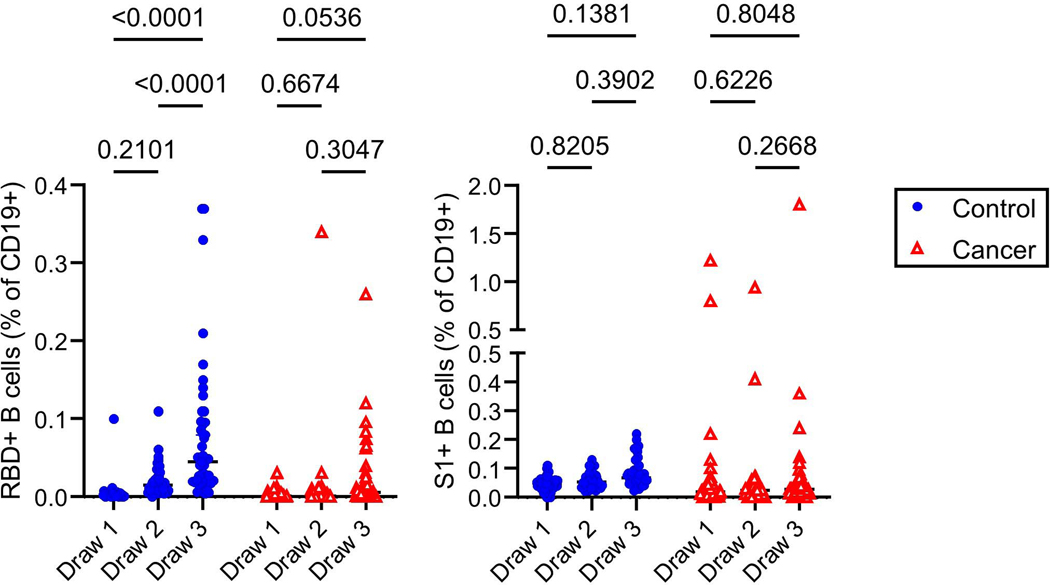
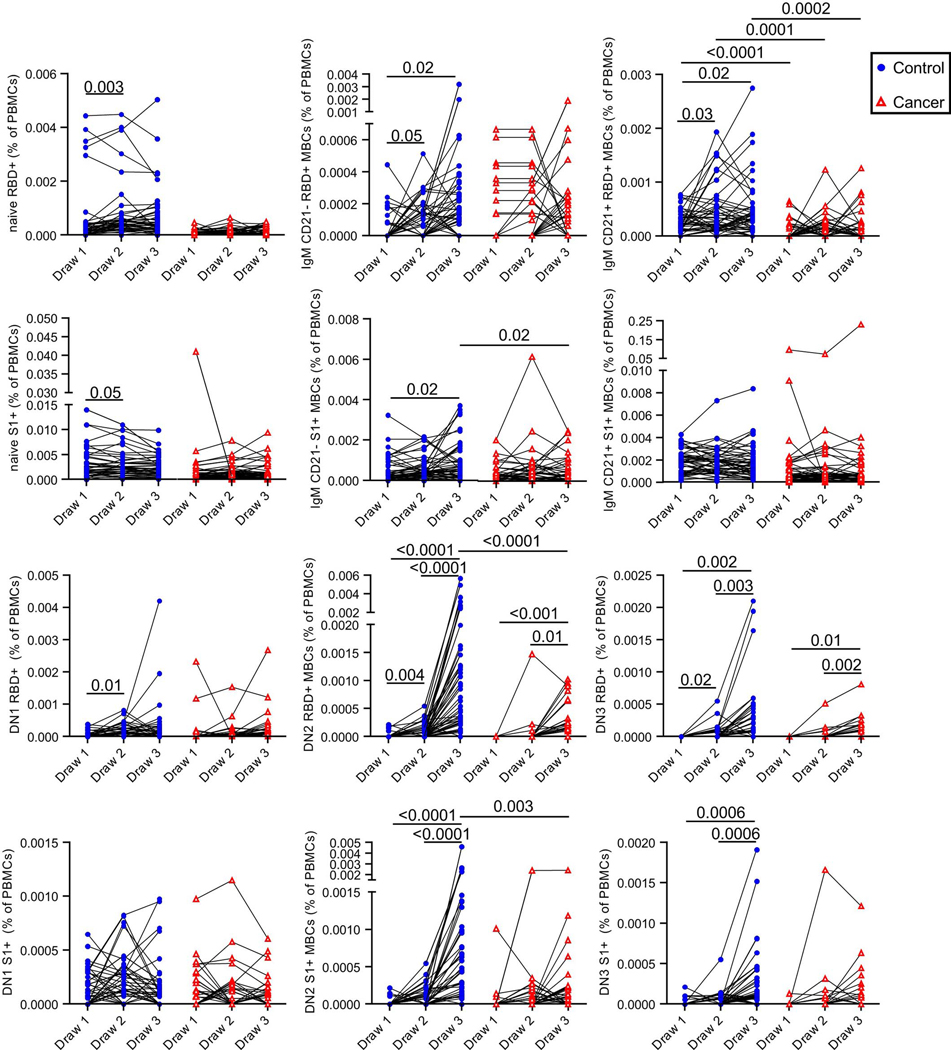
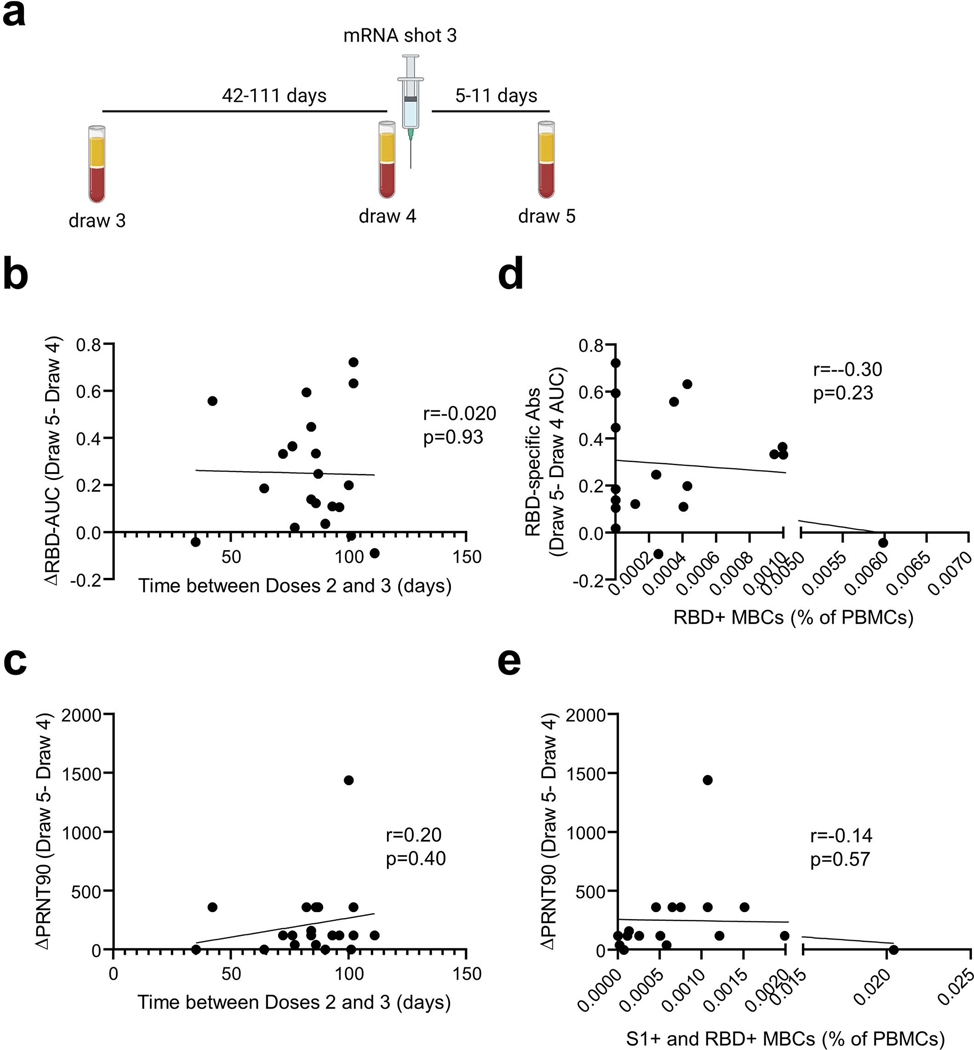
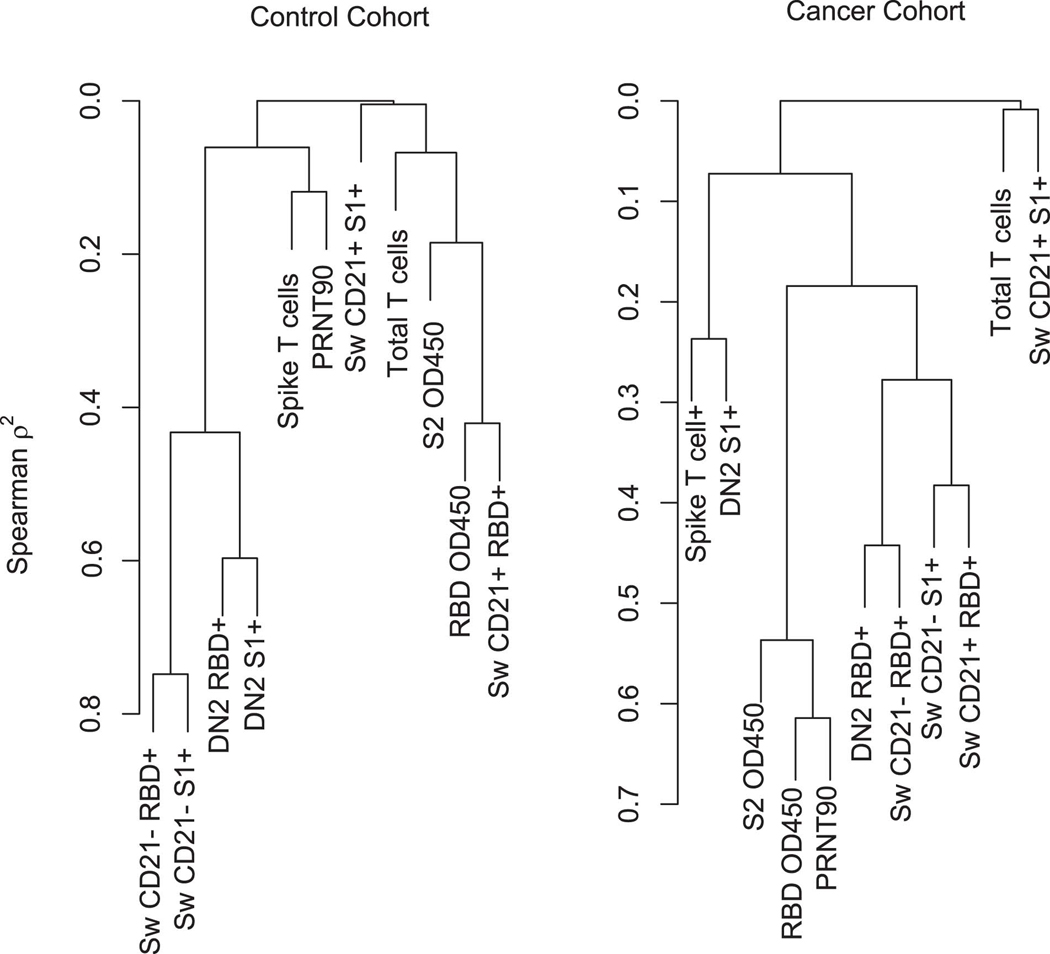
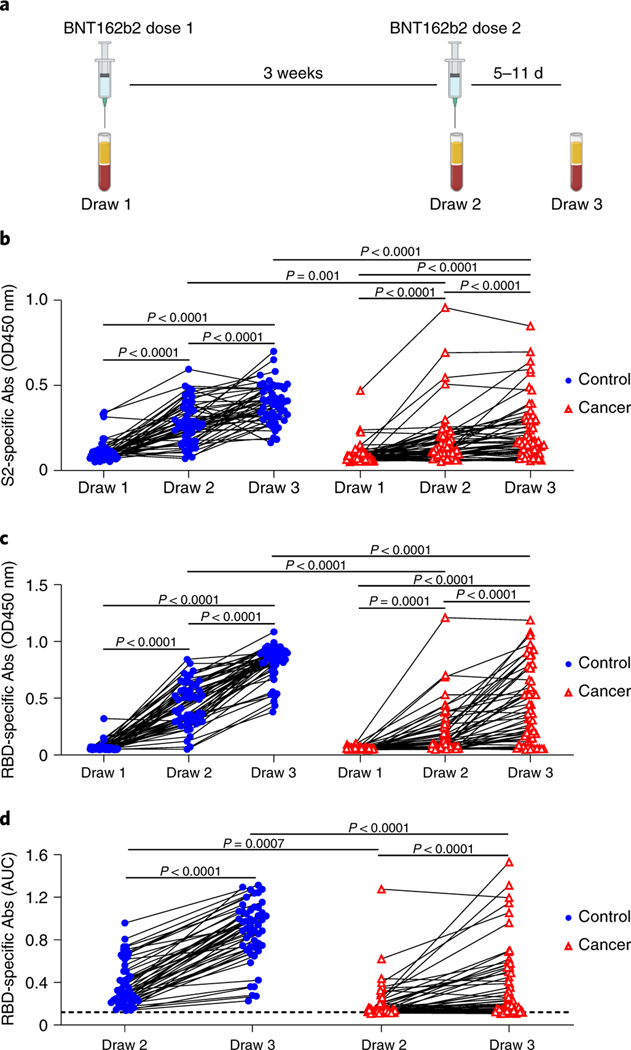
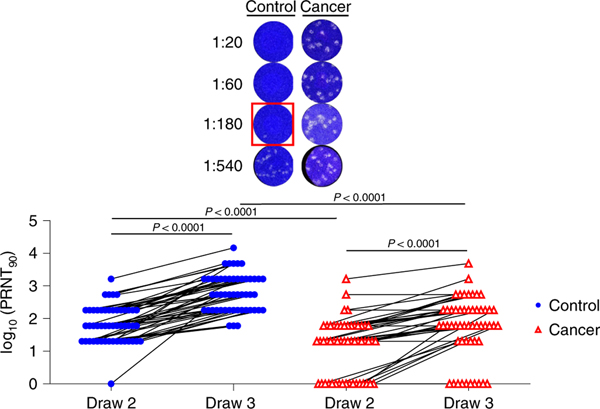
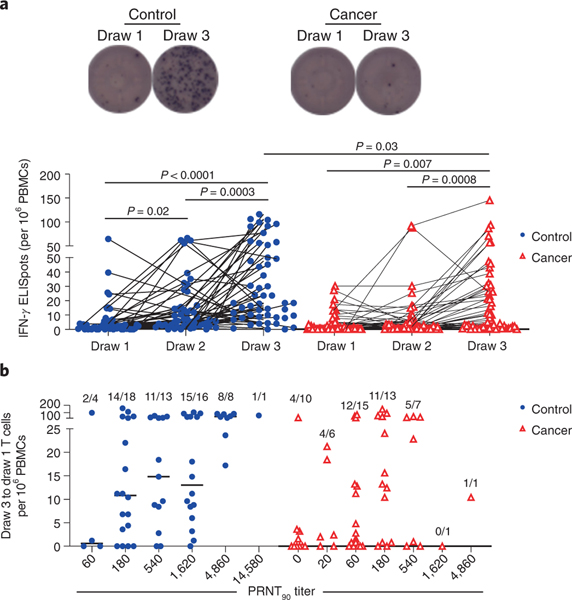
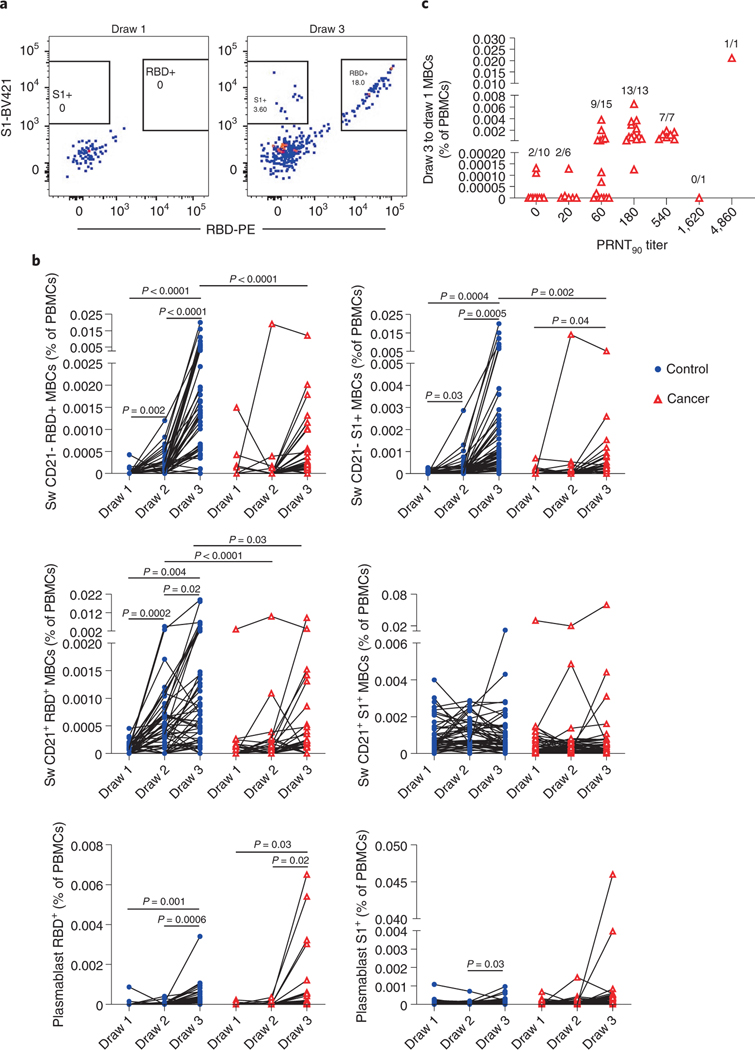
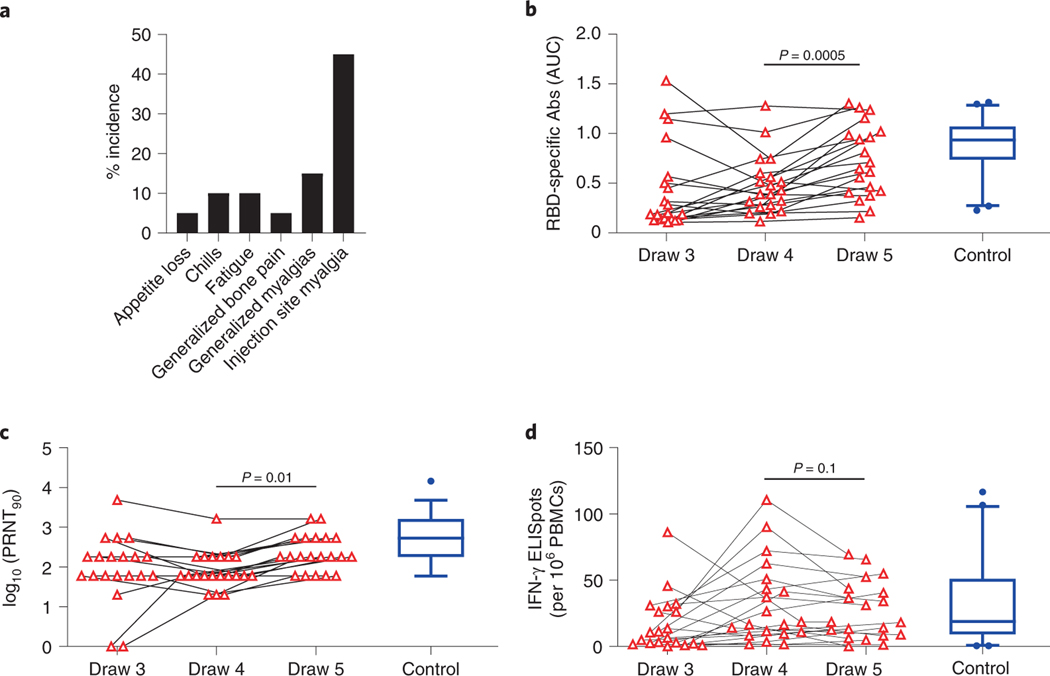
Vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have shown high efficacy, but immunocompromised participants were excluded from controlled clinical trials. In this study, we compared immune responses to the BNT162b2 mRNA Coronavirus Disease 2019 vaccine in patients with solid tumors (n = 53) who were on active cytotoxic anti-cancer therapy to a control cohort of participants without cancer (n = 50). Neutralizing antibodies were detected in 67% of patients with cancer after the first immunization, followed by a threefold increase in median titers after the second dose. Similar patterns were observed for spike protein-specific serum antibodies and T cells, but the magnitude of each of these responses was diminished relative to the control cohort. In most patients with cancer, we detected spike receptor-binding domain and other S1-specific memory B cell subsets as potential predictors of anamnestic responses to additional immunizations. We therefore initiated a phase 1 trial for 20 cancer cohort participants of a third vaccine dose of BNT162b2 ( NCT04936997 ); primary outcomes were immune responses, with a secondary outcome of safety. At 1 week after a third immunization, 16 participants demonstrated a median threefold increase in neutralizing antibody responses, but no improvement was observed in T cell responses. Adverse events were mild. These results suggest that a third dose of BNT162b2 is safe, improves humoral immunity against SARS-CoV-2 and could be immunologically beneficial for patients with cancer on active chemotherapy.
© 2021. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing interests:
The remaining authors declare no competing interests and no authors are employees of relevant companies.
Figures
Update of
-
Immune Responses to COVID-19 mRNA Vaccines in Patients with Solid Tumors on Active, Immunosuppressive Cancer Therapy.medRxiv [Preprint]. 2021 Aug 25:2021.05.13.21257129. doi: 10.1101/2021.05.13.21257129. medRxiv. 2021. Update in: Nat Med. 2021 Nov;27(11):2002-2011. doi: 10.1038/s41591-021-01542-z. PMID: 34013289 Free PMC article. Updated. Preprint.
Comment in
-
Boosting immunity to COVID-19 vaccines.Nat Med. 2021 Nov;27(11):1874-1875. doi: 10.1038/s41591-021-01560-x. Nat Med. 2021. PMID: 34764485 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
