

Sporadic Rift Valley Fever Outbreaks in Humans and Animals in Uganda, October 2017-January 2018
- PMID: 34594384
- PMCID: PMC8478567
- DOI: 10.1155/2021/8881191
Sporadic Rift Valley Fever Outbreaks in Humans and Animals in Uganda, October 2017-January 2018
Abstract
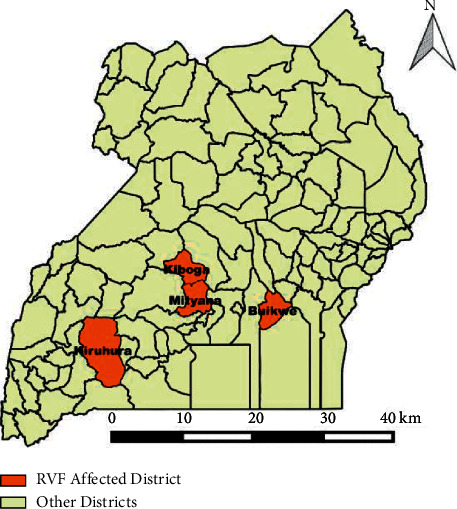
Introduction: Rift Valley fever (RVF) is a mosquito-borne viral zoonosis. The Uganda Ministry of Health received alerts of suspected viral haemorrhagic fever in humans from Kiruhura, Buikwe, Kiboga, and Mityana districts. Laboratory results from Uganda Virus Research Institute indicated that human cases were positive for Rift Valley fever virus (RVFV) by polymerase chain reaction. We investigated to determine the scope of outbreaks, identify exposure factors, and recommend evidence-based control and prevention measures.
Methods: A suspected case was defined as a person with acute fever onset, negative malaria test result, and at least two of the following symptoms: headache, muscle or joint pain, bleeding, and any gastroenteritis symptom (nausea, vomiting, abdominal pain, diarrhoea) in a resident of Kiruhura, Buikwe, Mityana, and Kiboga districts from 1st October 2017 to 30th January 2018. A confirmed case was defined as a suspected case with laboratory confirmation by either detection of RVF nucleic acid by reverse-transcriptase polymerase chain reaction (RT-PCR) or demonstration of serum IgM or IgG antibodies by ELISA. Community case finding was conducted in all affected districts. In-depth interviews were conducted with human cases that were infected with RVF who included herdsmen and slaughterers/meat handlers to identify exposure factors for RVF infection. A total of 24 human and 362 animal blood samples were tested. Animal blood samples were purposively collected from farms that had reported stormy abortions in livestock and unexplained death of animals after a short illness (107 cattle, 83 goats, and 43 sheep). Convenient sampling for the wildlife (10 zebras, 1 topi, and 1 impala) was conducted to investigate infection in animals from Kiruhura, Buikwe, Mityana, and Kiboga districts. Human blood was tested for anti-RVFV IgM and IgG and animal blood for anti-RVFV IgG. Environmental assessments were conducted during the outbreaks in all the affected districts.
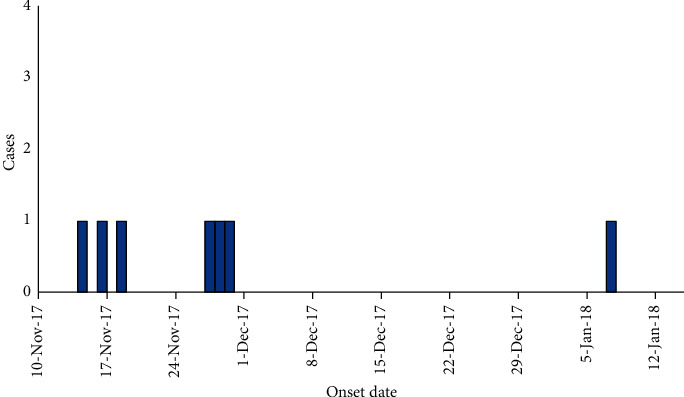
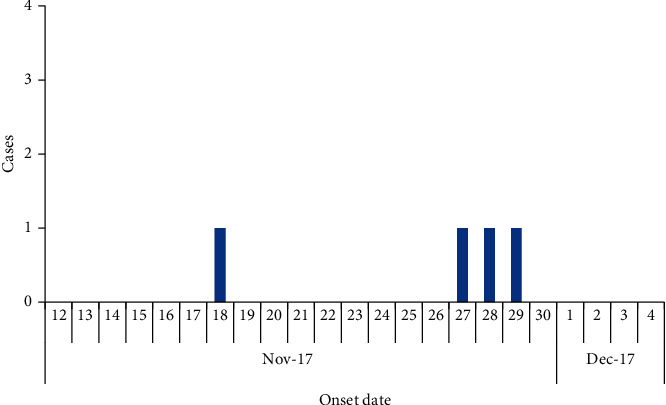
Results: Sporadic RVF outbreaks occurred from mid-October 2017 to mid-January 2018 affecting humans, domestic animals, and wildlife. Human cases were reported from Kiruhura, Buikwe, Kiboga, and Mityana districts. Of the 24 human blood samples tested, anti-RVFV IgG was detected in 7 (29%) human samples; 1 human sample had detectable IgM only, and 6 had both IgM and IgG. Three of the seven confirmed human cases died among humans. Results from testing animal blood samples obtained from Kiruhura district indicated that 44% (64/146) cattle, 46% (35/76) goats, and 45% (9/20) sheep tested positive for RVF. Among wildlife, (1/10) zebras, (1/1) topi, and (1/1) impala tested positive for RVFV by serological tests. One blood sample from sheep in Kiboga district tested RVFV positive. All the human cases were exposed through contact or consumption of meat from infected animals.
Conclusion: RVF outbreaks occurred in humans and animals in Kiruhura, Buikwe, Mityana, and Kiboga districts. Human cases were potentially infected through contact with infected animals and their products.
Copyright © 2021 Doreen Birungi et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Prevalence and risk factors of Rift Valley fever in humans and animals from Kabale district in Southwestern Uganda, 2016.PLoS Negl Trop Dis. 2018 May 3;12(5):e0006412. doi: 10.1371/journal.pntd.0006412. eCollection 2018 May. PLoS Negl Trop Dis. 2018. PMID: 29723189 Free PMC article.
-
Rift valley fever outbreak in Sembabule District, Uganda, December 2020.One Health Outlook. 2023 Nov 27;5(1):16. doi: 10.1186/s42522-023-00092-3. One Health Outlook. 2023. PMID: 38012800 Free PMC article.
-
Serological evidence of Rift Valley fever virus infection among domestic ruminant herds in Uganda.BMC Vet Res. 2021 Apr 13;17(1):157. doi: 10.1186/s12917-021-02867-0. BMC Vet Res. 2021. PMID: 33849526 Free PMC article.
-
Rift Valley Fever: An Emerging Mosquito-Borne Disease.Annu Rev Entomol. 2016;61:395-415. doi: 10.1146/annurev-ento-010715-023819. Annu Rev Entomol. 2016. PMID: 26982443 Review.
-
Rift Valley Fever.Vet Clin North Am Food Anim Pract. 2024 Jul;40(2):293-304. doi: 10.1016/j.cvfa.2024.01.004. Epub 2024 Mar 6. Vet Clin North Am Food Anim Pract. 2024. PMID: 38453549 Review.
Cited by
-
Severe morbidity and hospital-based mortality from Rift Valley fever disease between November 2017 and March 2020 among humans in Uganda.Virol J. 2024 May 3;21(1):104. doi: 10.1186/s12985-024-02377-z. Virol J. 2024. PMID: 38702807 Free PMC article.
-
Rift Valley Fever Outbreak during COVID-19 Surge, Uganda, 2021.Emerg Infect Dis. 2022 Nov;28(11):2290-2293. doi: 10.3201/eid2811.220364. Epub 2022 Sep 23. Emerg Infect Dis. 2022. PMID: 36150455 Free PMC article.
-
Human and Livestock Surveillance Revealed the Circulation of Rift Valley Fever Virus in Agnam, Northern Senegal, 2021.Trop Med Infect Dis. 2023 Jan 27;8(2):87. doi: 10.3390/tropicalmed8020087. Trop Med Infect Dis. 2023. PMID: 36828503 Free PMC article.
-
Spatial and temporal analysis of Rift Valley fever outbreaks in livestock in Uganda: a retrospective study from 2013 to 2022.BMC Vet Res. 2025 May 26;21(1):375. doi: 10.1186/s12917-025-04825-6. BMC Vet Res. 2025. PMID: 40420030 Free PMC article.
-
The Re-Emergence of Rift Valley Fever in Mananjary District, Madagascar in 2021: A Call for Action.Pathogens. 2024 Mar 16;13(3):257. doi: 10.3390/pathogens13030257. Pathogens. 2024. PMID: 38535600 Free PMC article.
References
-
- Daubney R., Hudson J. R., Garnham P. C. Enzootic hepatitis or Rift Valley fever. An undescribed virus disease of sheep cattle and man from East Africa. Journal of Pathology & Bacteriology . 1931;34(4):545–579. doi: 10.1002/path.1700340418. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
