Diagnostic Value of Straight Head Hanging in Posterior Canal Benign Paroxysmal Positional Vertigo
- PMID: 34595864
- PMCID: PMC8490902
- DOI: 10.3988/jcn.2021.17.4.558
Diagnostic Value of Straight Head Hanging in Posterior Canal Benign Paroxysmal Positional Vertigo
Abstract
Background and purpose: To determine the diagnostic value of straight head hanging (SHH) in benign paroxysmal positional vertigo involving the posterior semicircular canal (PC-BPPV).
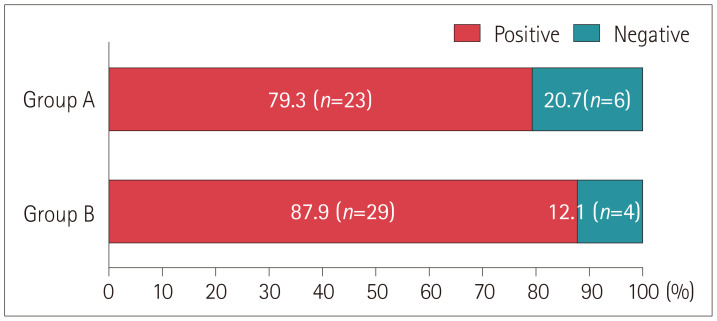
Methods: We retrospectively included 62 patients (age=56.2±15.0 years, 47 female) with unilateral PC-BPPV who underwent both the Dix-Hallpike maneuver and SHH before receiving canalith repositioning therapy (CRT) between September 2017 and July 2020 at the Dizziness Center of Seoul National University Bundang Hospital in South Korea (16 patients, 25.8%) or the Neurology Outpatient Clinic of Aerospace Central Hospital in China (46 patients, 74.2%). SHH was performed before (n=29, group A) or after (n=33, group B) the Dix-Hallpike maneuver.
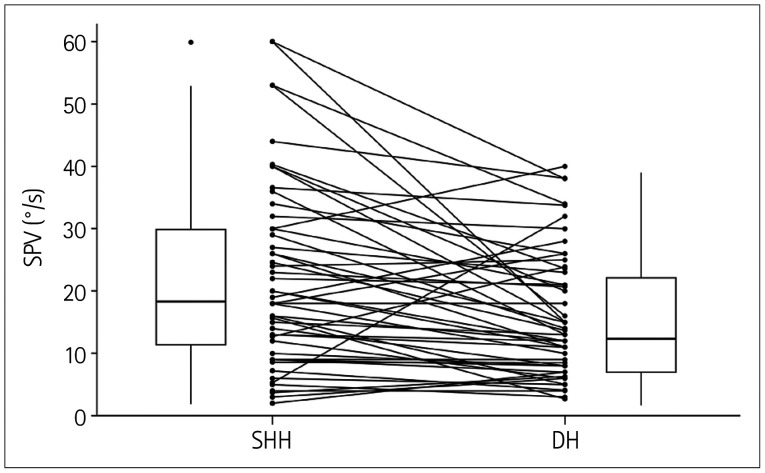
Results: Torsional upbeat nystagmus typical of PC-BPPV was induced during SHH in 52 (83.9%) patients, and the incidence of this type of positional nystagmus did not differ between the groups A and B (79.3% vs. 87.9%, p=0.569). The maximum slow-phase velocity of the induced upbeat nystagmus was higher during SHH than during the Dix-Hallpike maneuver toward the lesion side [range=2.0-60.0°/s (median=18.5°/s) vs. range=2.7-40.0°/s (median=13.4°/s), p<0.001]. Reversal of the positional nystagmus was observed upon resuming the sitting position after SHH in 47 (75.8%) patients and after the Dix-Hallpike maneuver in 54 (87.7%) patients, with no significant difference between the groups (p=0.082).
Conclusions: SHH is effective for diagnosing PC-BPPV. Given its simplicity, SHH may be performed before the Dix-Hallpike maneuver, and CRT may be attempted thereafter when the typical positional nystagmus for unilateral PC-BPPV is induced during SHH.
Keywords: benign paroxysmal positional vertigo; dizziness; nystagmus; vertigo.
Copyright © 2021 Korean Neurological Association.
Conflict of interest statement
Ji-Soo Kim and Jeong-Yoon Choi, a contributing editor of the Journal of Clinical Neurology, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Figures
Similar articles
-
Clinical Application of Different Vertical Position Tests for Posterior Canal-Benign Paroxysmal Positional Vertigo-Cupulolithiasis.Front Neurol. 2022 Jul 12;13:930542. doi: 10.3389/fneur.2022.930542. eCollection 2022. Front Neurol. 2022. PMID: 35903115 Free PMC article.
-
"Sitting-up vertigo as an expression of posterior semicircular canal heavy cupula and posterior semicircular canal short arm canalolithiasis".J Otol. 2022 Apr;17(2):101-106. doi: 10.1016/j.joto.2022.02.001. Epub 2022 Feb 16. J Otol. 2022. PMID: 35949549 Free PMC article.
-
Retrospective analysis of nystagmus characteristics and clinical applications of positional testing in patients with cupulolithiasis of the posterior semicircular canal in benign paroxysmal positional vertigo.Front Neurol. 2024 Jul 10;15:1413929. doi: 10.3389/fneur.2024.1413929. eCollection 2024. Front Neurol. 2024. PMID: 39050123 Free PMC article.
-
Classification, diagnostic criteria and management of benign paroxysmal positional vertigo.Auris Nasus Larynx. 2017 Feb;44(1):1-6. doi: 10.1016/j.anl.2016.03.013. Epub 2016 May 9. Auris Nasus Larynx. 2017. PMID: 27174206 Review.
-
[Benign paroxysmal positional vertigo: who can diagnose it, how should it be treated and where?].Harefuah. 2005 Aug;144(8):567-71, 597. Harefuah. 2005. PMID: 16146156 Review. Hebrew.
Cited by
-
Rapid axial roll test outperforms alternative positional tests in identifying the affected ear in HSC-BPPV: an observational cohort study.Front Neurol. 2024 Jun 19;15:1432608. doi: 10.3389/fneur.2024.1432608. eCollection 2024. Front Neurol. 2024. PMID: 38962475 Free PMC article.
-
Identifying tests to evaluate in a diagnostic accuracy study for patients with vertigo in general practice: a Delphi study.BMC Prim Care. 2025 Aug 2;26(1):238. doi: 10.1186/s12875-025-02920-z. BMC Prim Care. 2025. PMID: 40753388 Free PMC article.
-
Upbeat and Direction-Changing Torsional Nystagmus While Straight Head Hanging: A New Sign of Benign Paroxysmal Positional Vertigo Involving Bilateral Posterior Semicircular Canals.J Clin Neurol. 2024 Jan;20(1):100-102. doi: 10.3988/jcn.2023.0299. J Clin Neurol. 2024. PMID: 38179639 Free PMC article. No abstract available.
-
Canal switch in benign paroxysmal positional vertigo: Clinical characteristics and possible mechanisms.Front Neurol. 2022 Nov 14;13:1049828. doi: 10.3389/fneur.2022.1049828. eCollection 2022. Front Neurol. 2022. PMID: 36452167 Free PMC article.
References
-
- Baloh RW, Sakala SM, Honrubia V. Benign paroxysmal positional nystagmus. Am J Otolaryngol. 1979;1:1–6. - PubMed
-
- McClure JA. Horizontal canal BPV. J Otolaryngol. 1985;14:30–35. - PubMed
-
- Gresty MA, Bronstein AM, Brandt T, Dieterich M. Neurology of otolith function. Peripheral and central disorders. Brain. 1992;115:647–673. - PubMed
-
- Kim JS, Zee DS. Clinical practice. Benign paroxysmal positional vertigo. N Engl J Med. 2014;370:1138–1147. - PubMed
-
- von Brevern M, Bertholon P, Brandt T, Fife T, Imai T, Nuti D, et al. Benign paroxysmal positional vertigo: diagnostic criteria. J Vestib Res. 2015;25:105–117. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials