

Characterizing demographics, comorbidities, and costs of care among populations with Duchenne muscular dystrophy with Medicaid and commercial coverage
- PMID: 34595954
- PMCID: PMC10391028
- DOI: 10.18553/jmcp.2021.27.10.1426
Characterizing demographics, comorbidities, and costs of care among populations with Duchenne muscular dystrophy with Medicaid and commercial coverage
Abstract
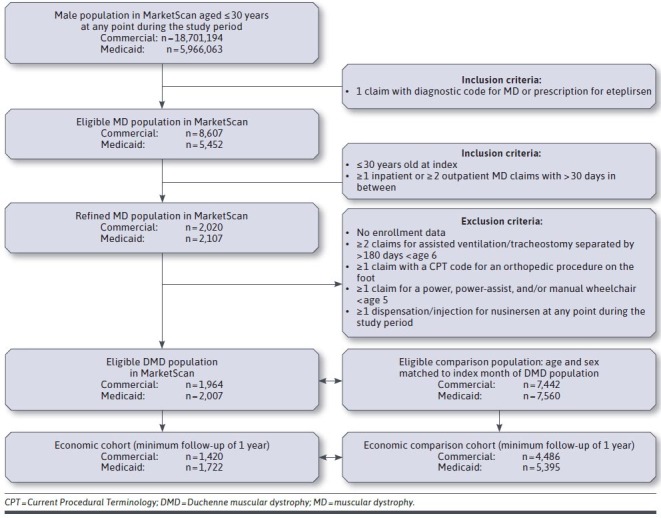
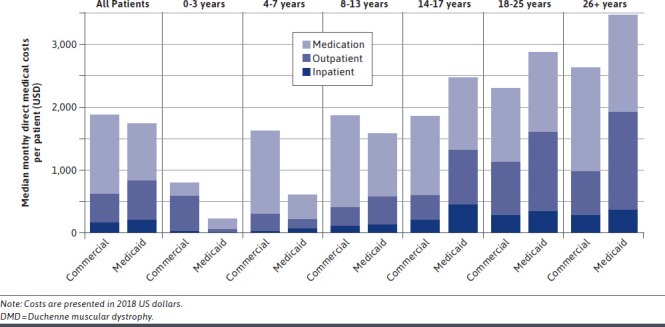
BACKGROUND: Duchenne muscular dystrophy (DMD) is a severe X-linked progressive neurodegenerative disease characterized by loss of ambulation, cardiomyopathy, respiratory insufficiency, and early mortality. Few data are available that describe the direct medical costs among patients with DMD in the United States. OBJECTIVE: To characterize the demographics, comorbidity burden, and direct monthly costs of care among patients with DMD with Medicaid and with commercial insurance coverage. METHODS: IBM MarketScan Commercial and Multi-State Medicaid claims (2013-2018) were used to identify males aged 30 years or under with diagnostic codes for muscular dystrophy or DMD; additional exclusion criteria were applied to identify those with probable DMD. Baseline characteristics and comorbidities were tabulated. The frequency of health care resource use and median (interquartile range [IQR]) monthly costs (in 2018 USD) were estimated from those with at least 12 months of continuous follow-up. RESULTS: Median (IQR) baseline ages were similar between the Medicaid (14 [9-20] years; n = 2,007) and commercial (15 [9-21] years; n = 1,964) DMD cohorts. The frequency of comorbidities over the period was slightly higher with those on Medicaid. The median duration of follow-up was 3.1 years among members of the Medicaid DMD cohort and 1.7 years among the commercial DMD cohort. Median monthly resource use was generally higher among the Medicaid DMD cohort; nonetheless, median (IQR) monthly costs were similar at $1,735 ($367-$5,281) for the Medicaid DMD cohort vs $1,883 ($657-$6,796) for the commercial DMD cohort. CONCLUSIONS: The demographic characteristics and median direct medical costs were similar between patients with commercial vs Medicaid coverage, even though patients with Medicaid coverage had higher resource use. Despite challenges in definitively identifying DMD patients using claims data, these findings help characterize contemporary DMD populations in the United States and the related direct economic burden to the payer. DISCLOSURES: This study was funded by Sarepta Therapeutics, Inc. Klimchak and Gooch are employees of Sarepta Therapeutics Inc. Szabo, Qian, and Popoff are employees of Broadstreet HEOR, which received funds from Sarepta Therapeutics, Inc., for work on this study. Iannaccone has received research funding or consulting fees from Avexis, Biogen, Fibrogen, Mallinkrodt, Regeneron, Sarepta Therapeutics, Inc., Scholar Rock, PTC Therapeutics, Pfizer, MDA, CureSMA, NIH, Genentech-Roche, and BCBS. Publication of the study results was not contingent on the sponsor's approval or censorship of the manuscript. Information from this study was presented, in part, at the AMCP Virtual Annual Meeting, April 21-24, 2020.
Conflict of interest statement
This study was funded by Sarepta Therapeutics, Inc. Klimchak and Gooch are employees of Sarepta Therapeutics Inc. Szabo, Qian, and Popoff are employees of Broadstreet HEOR, which received funds from Sarepta Therapeutics, Inc., for work on this study. Iannaccone has received research funding or consulting fees from Avexis, Biogen, Fibrogen, Mallinkrodt, Regeneron, Sarepta Therapeutics, Inc., Scholar Rock, PTC Therapeutics, Pfizer, MDA, CureSMA, NIH, Genentech-Roche, and BCBS. Publication of the study results was not contingent on the sponsor’s approval or censorship of the manuscript.
Information from this study was presented, in part, at the AMCP Virtual Annual Meeting, April 21-24, 2020.
Figures
References
-
- Wein N, Alfano L, Flanigan KM. Genetics and emerging treatments for Duchenne and Becker muscular dystrophy. Pediatr Clin North Am. 2015;62(3):723-42. - PubMed
-
- Yiu EM, Kornberg AJ. Duchenne muscular dystrophy. J Paediatr Child Health. 2015;51(8):759-64. - PubMed
-
- Mirski KT, Crawford TO. Motor and cognitive delay in Duchenne muscular dystrophy: implication for early diagnosis. J Pediatr. 2014;165(5):1008-10. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
