

Cusp Overlap Technique: Should It Become the Standard Implantation Technique for Self-expanding Valves?
- PMID: 34599425
- PMCID: PMC8845572
- DOI: 10.1007/s11886-021-01583-3
Cusp Overlap Technique: Should It Become the Standard Implantation Technique for Self-expanding Valves?
Abstract
Purpose of review: Accurate imaging of the aortic root during valve implantation is crucial for proper prosthesis positioning during TAVR. The purpose of this review was to determine if routine use of the cusp-overlap view should be adopted for self-expanding valves.
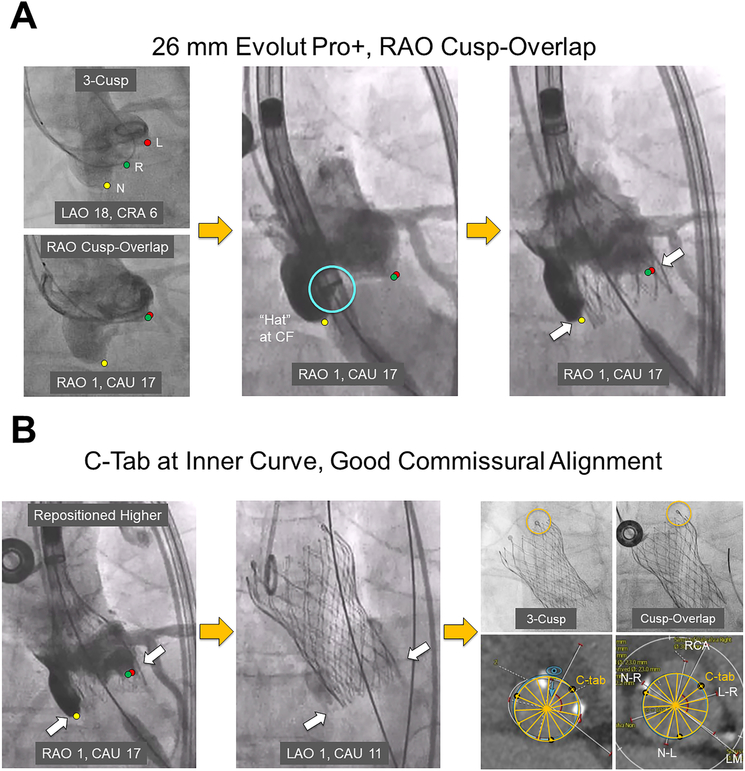
Recent findings: The use of the cusp-overlap view with the Evolut, Portico, ACURATE neo/neo2, and JenaValve systems is associated with lower post-procedural new permanent pacemaker implantation rates when compared with the standard 3-cusp view, presumably due to more precise valve implantation relative to the conduction system by the non-coronary cusp. By elongating the left ventricular outflow tract and accentuating the right-non commissure in the center of the fluoroscopic view, the cusp-overlap technique allows operators to more precisely control the prosthesis implant depth during self-expanding valve deployment. While the early experience with this approach in Evolut TAVR has been promising, the results of larger studies with longer follow-up across multiple self-expanding systems are warranted.
Keywords: Aortic stenosis; Commissural alignment; Cusp-overlap; Permanent pacemaker implantation; Self-expanding; Transcatheter aortic valve replacement.
© 2021. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Compliance with Ethical Standards
Conflict of Interest
Dr. Khera is a consultant for Abbott Structural Heart, Medtronic, and Boston Scientific, and has received speakers’ honoraria from Medtronic. Dr. Dangas is on the advisory board and is a consultant for Boston Scientific, and has common stock with Medtronic that is fully divested. Dr. Sharma has served on the Speakers Bureau for Abbott Vascular, Boston Scientific, TriReme, and Cardiovascular Systems. Dr. Tang has served as a physician proctor for Medtronic, and is a consultant for Medtronic and Abbott Structural Heart. The other authors have no conflicts of interest to declare.
Figures
References
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143(5):e72–e227. doi:10.1161/CIR.0000000000000923. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
