

Risk of cardiovascular disease in patients with fatty liver disease as defined from the metabolic dysfunction associated fatty liver disease or nonalcoholic fatty liver disease point of view: a retrospective nationwide claims database study in Japan
- PMID: 34601620
- PMCID: PMC8531127
- DOI: 10.1007/s00535-021-01828-6
Risk of cardiovascular disease in patients with fatty liver disease as defined from the metabolic dysfunction associated fatty liver disease or nonalcoholic fatty liver disease point of view: a retrospective nationwide claims database study in Japan
Abstract
Background: Nonalcoholic fatty liver disease (NAFLD) and metabolic dysfunction associated fatty liver disease (MAFLD) have important associations with cardiovascular disease (CVD). The main objective of this study was to compare the frequency of incidence rate of CVD in the NAFLD or MAFLD patients utilizing a large claims database.
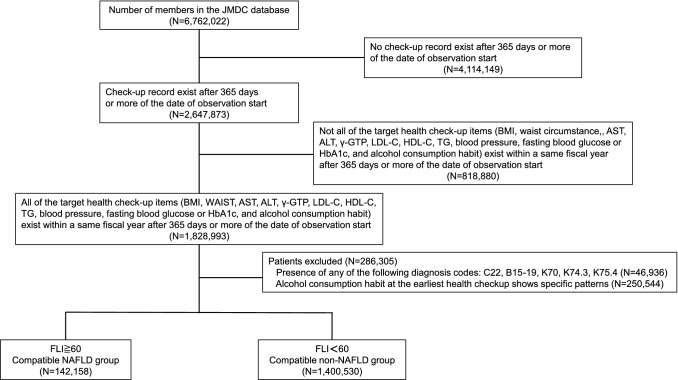
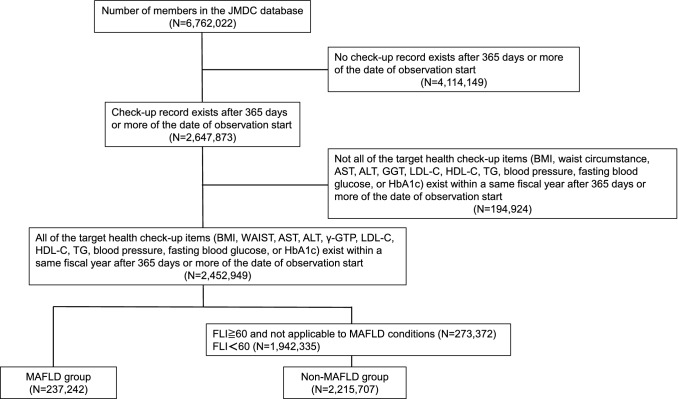
Methods: Using the JMDC database from April 2013 to March 2019, we retrospectively analyzed data for 1,542,688 and 2,452,949 people to estimate the relationship between CVD and NAFLD, MAFLD, respectively.
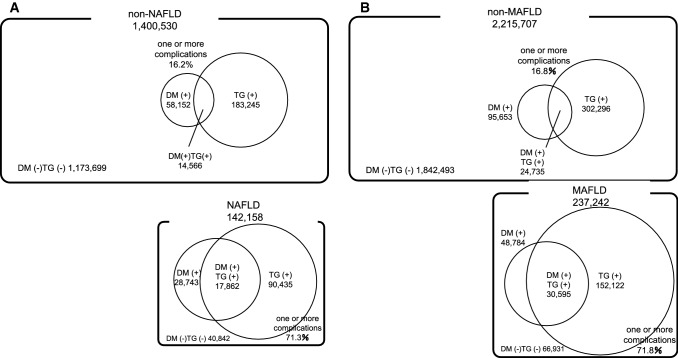
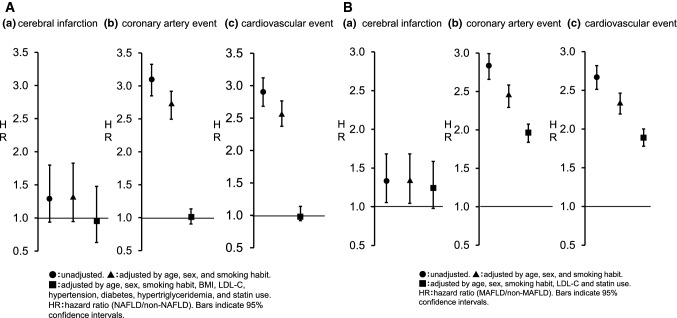
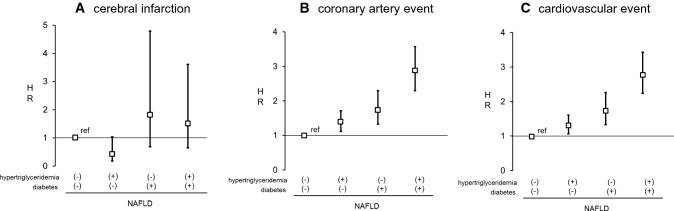
Results: The incidence rates of CVD were 0.97 (95% CI 0.94-1.01) and 2.82 (95% CI 2.64-3.01) per 1000 person-years in the non-NAFLD and NAFLD groups, respectively, and 1.01 (95% CI 0.98-1.03) and 2.69 (95% CI 2.55-2.83) per 1000 person-years in the non-MAFLD and MAFLD groups, respectively. The overall prevalence of hypertriglyceridemia and diabetes mellitus (DM) was 13.1, and 4.2%, respectively, in the non-NAFLD group and 63.6, and 20.2%, respectively, in the NAFLD group. The overall prevalenceof hypertriglyceridemia and DM was 13.6 and 4.3%, respectively, in the non-MAFLD group and 64.1, and 20.6%, respectively, in the MAFLD group. HRs for CVD increased with hypertriglyceridemia and DM.
Conclusions: Results indicated that incident rate of CVD increased with NAFLD/MAFLD; the complication rate of DM and hypertriglyceridemia among NAFLD/MAFLD patients is high and may affect the development of CVD.
Keywords: Cardiovascular disease; Diabetes mellitus; Hypertriglyceridemia; Metabolic dysfunction associated fatty liver disease; Non-alcoholic fatty liver disease.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
