

Differential chemokine alteration in the variants of primary progressive aphasia-a role for neuroinflammation
- PMID: 34602080
- PMCID: PMC8489077
- DOI: 10.1186/s12974-021-02247-3
Differential chemokine alteration in the variants of primary progressive aphasia-a role for neuroinflammation
Abstract
Background: The primary progressive aphasias (PPA) represent a group of usually sporadic neurodegenerative disorders with three main variants: the nonfluent or agrammatic variant (nfvPPA), the semantic variant (svPPA), and the logopenic variant (lvPPA). They are usually associated with a specific underlying pathology: nfvPPA with a primary tauopathy, svPPA with a TDP-43 proteinopathy, and lvPPA with underlying Alzheimer's disease (AD). Little is known about their cause or pathophysiology, but prior studies in both AD and svPPA have suggested a role for neuroinflammation. In this study, we set out to investigate the role of chemokines across the PPA spectrum, with a primary focus on central changes in cerebrospinal fluid (CSF) METHODS: Thirty-six participants with sporadic PPA (11 svPPA, 13 nfvPPA, and 12 lvPPA) as well as 19 healthy controls were recruited to the study and donated CSF and plasma samples. All patients with lvPPA had a tau/Aβ42 biomarker profile consistent with AD, whilst this was normal in the other PPA groups and controls. We assessed twenty chemokines in CSF and plasma using Proximity Extension Assay technology: CCL2 (MCP-1), CCL3 (MIP-1a), CCL4 (MIP-1β), CCL7 (MCP-3), CCL8 (MCP-2), CCL11 (eotaxin), CCL13 (MCP-4), CCL19, CCL20, CCL23, CCL25, CCL28, CX3CL1 (fractalkine), CXCL1, CXCL5, CXCL6, CXCL8 (IL-8), CXCL9, CXCL10, and CXCL11.
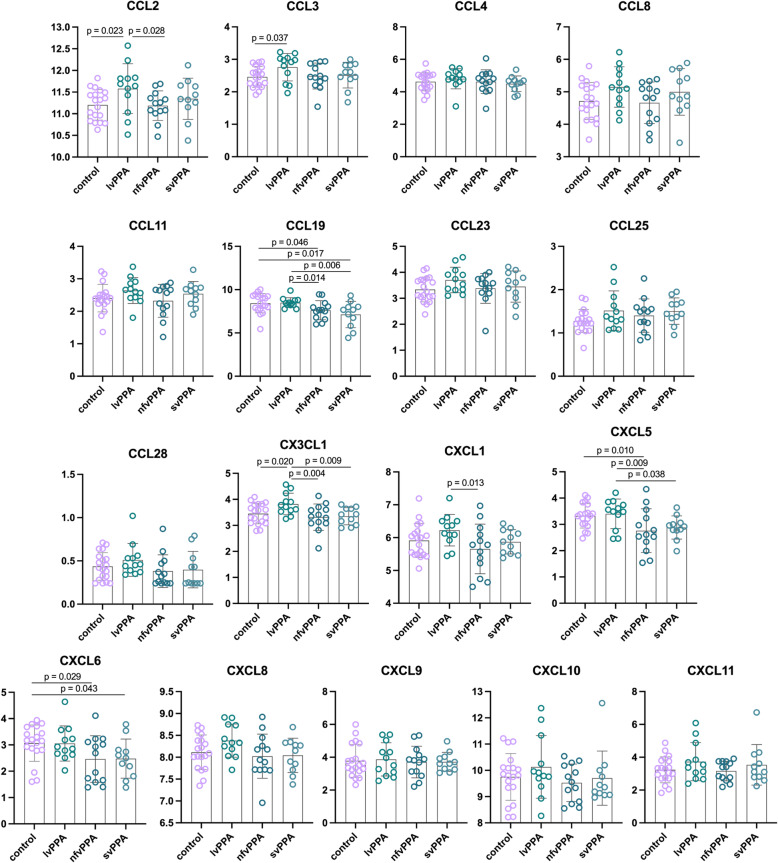
Results: In CSF, CCL19 and CXCL6 were decreased in both svPPA and nfvPPA compared with controls whilst CXCL5 was decreased in the nfvPPA group with a borderline significant decrease in the svPPA group. In contrast, CCL2, CCL3 and CX3CL1 were increased in lvPPA compared with controls and nfvPPA (and greater than svPPA for CX3CL1). CXCL1 was also increased in lvPPA compared with nfvPPA but not the other groups. CX3CL1 was significantly correlated with CSF total tau concentrations in the controls and each of the PPA groups. Fewer significant differences were seen between groups in plasma, although in general, results were in the opposite direction to CSF, i.e. decreased in lvPPA compared with controls (CCL3 and CCL19), and increased in svPPA (CCL8) and nfvPPA (CCL13).
Conclusion: Differential alteration of chemokines across the PPA variants is seen in both CSF and plasma. Importantly, these results suggest a role for neuroinflammation in these poorly understood sporadic disorders, and therefore also a potential future therapeutic target.
Keywords: Chemokines; Frontotemporal dementia; Primary progressive aphasia.
© 2021. The Author(s).
Conflict of interest statement
HZ has served at scientific advisory boards for Eisai, Denali, Roche Diagnostics, Wave, Samumed, Siemens Healthineers, Pinteon Therapeutics, Nervgen, AZTherapies, and CogRx, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure, and Biogen, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program. JDR has served on medical advisory boards and undertaken consultancy for Alector, Arkuda Therapeutics, Wave Life Sciences, and Prevail Therapeutics. He has also undertaken consultancy for UCB, AC Immune, Astex Pharmaceuticals, Biogen, Takeda and Eisai.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
