

Deep-learning model for screening sepsis using electrocardiography
- PMID: 34602084
- PMCID: PMC8487616
- DOI: 10.1186/s13049-021-00953-8
Deep-learning model for screening sepsis using electrocardiography
Abstract
Background: Sepsis is a life-threatening organ dysfunction and a major healthcare burden worldwide. Although sepsis is a medical emergency that requires immediate management, screening for the occurrence of sepsis is difficult. Herein, we propose a deep learning-based model (DLM) for screening sepsis using electrocardiography (ECG).
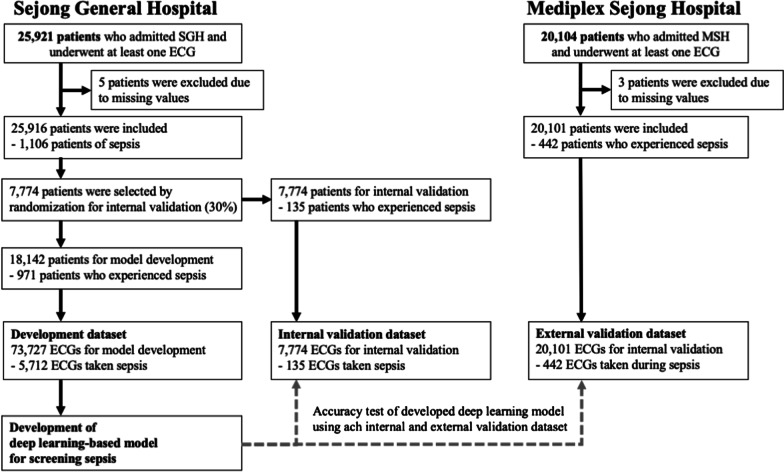
Methods: This retrospective cohort study included 46,017 patients who were admitted to two hospitals. A total of 1,548 and 639 patients had sepsis and septic shock, respectively. The DLM was developed using 73,727 ECGs from 18,142 patients, and internal validation was conducted using 7774 ECGs from 7,774 patients. Furthermore, we conducted an external validation with 20,101 ECGs from 20,101 patients from another hospital to verify the applicability of the DLM across centers.
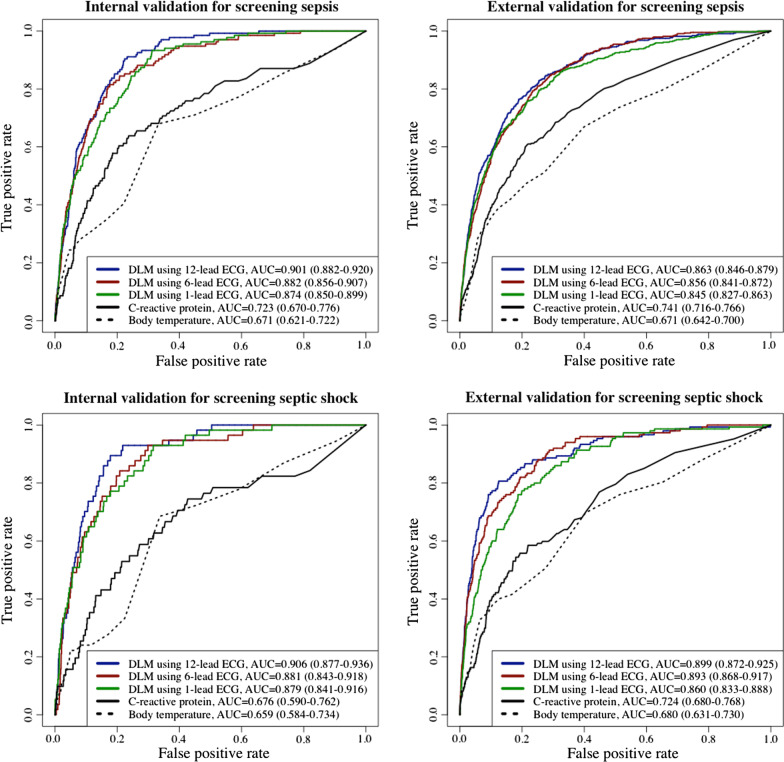
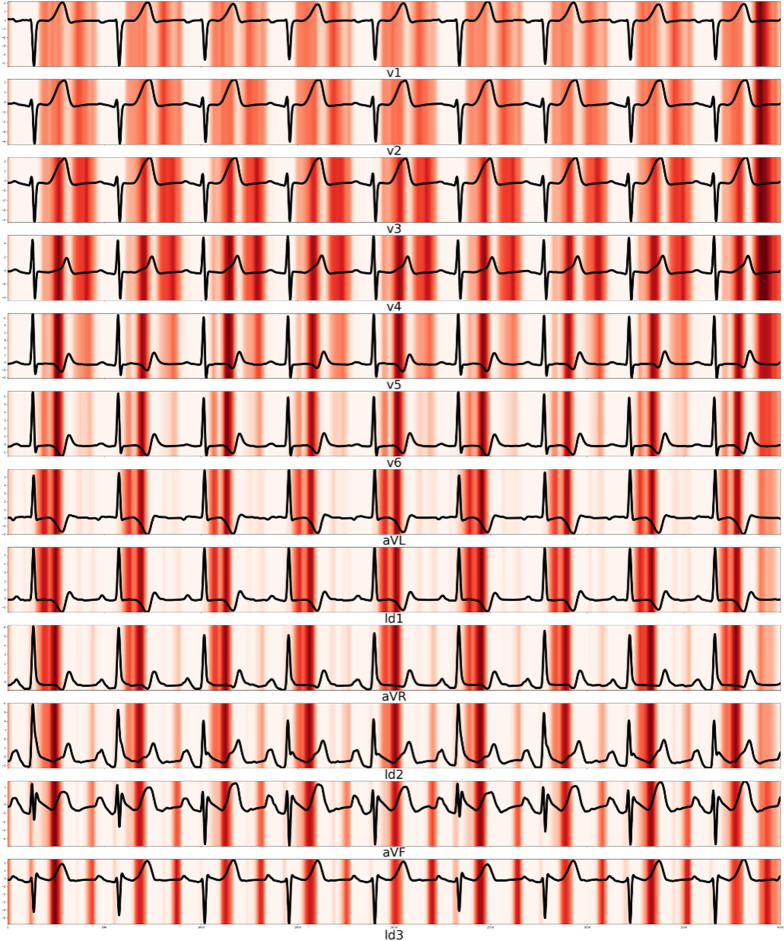
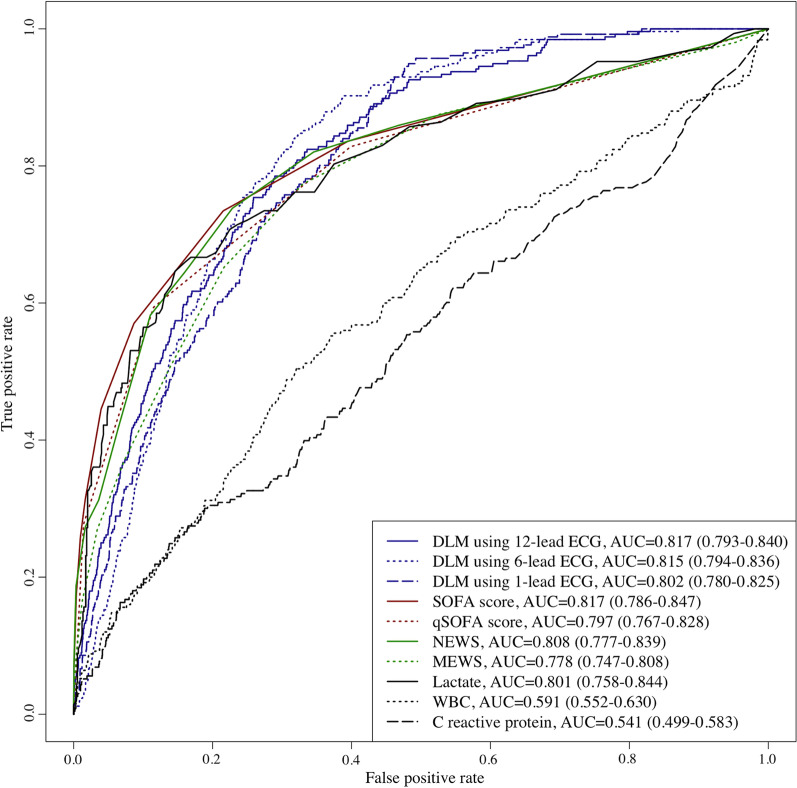
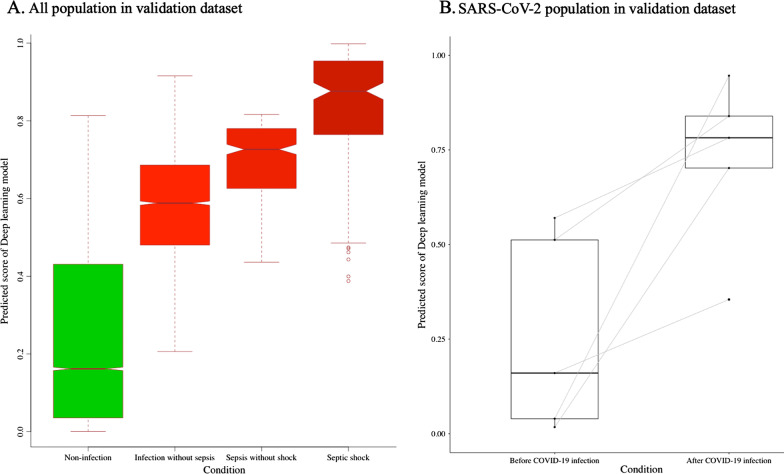
Results: During the internal and external validations, the area under the receiver operating characteristic curve (AUC) of the DLM using 12-lead ECG was 0.901 (95% confidence interval, 0.882-0.920) and 0.863 (0.846-0.879), respectively, for screening sepsis and 0.906 (95% confidence interval (CI), 0.877-0.936) and 0.899 (95% CI, 0.872-0.925), respectively, for detecting septic shock. The AUC of the DLM for detecting sepsis using 6-lead and single-lead ECGs was 0.845-0.882. A sensitivity map revealed that the QRS complex and T waves were associated with sepsis. Subgroup analysis was conducted using ECGs from 4,609 patients who were admitted with an infectious disease, and the AUC of the DLM for predicting in-hospital mortality was 0.817 (0.793-0.840). There was a significant difference in the prediction score of DLM using ECG according to the presence of infection in the validation dataset (0.277 vs. 0.574, p < 0.001), including severe acute respiratory syndrome coronavirus 2 (0.260 vs. 0.725, p = 0.018).
Conclusions: The DLM delivered reasonable performance for sepsis screening using 12-, 6-, and single-lead ECGs. The results suggest that sepsis can be screened using not only conventional ECG devices but also diverse life-type ECG machines employing the DLM, thereby preventing irreversible disease progression and mortality.
Keywords: Artificial intelligence; Deep learning; Electrocardiography; Infections; Sepsis; Shock, Septic.
© 2021. The Author(s).
Conflict of interest statement
YRL, DYK, KHK, and SYL declare that they have no competing interests. JK, YYJ, MSJ, YJL, YHC, and JHS are researchers of Medical AI Co., a medical artificial intelligence company. JK and JHB are the researchers of Body Friend Co. There are no products in development or marketed products to declare. This does not alter our adherence to the target journal.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
