

A Multimodal Risk Network Predicts Executive Function Trajectories in Non-demented Aging
- PMID: 34603005
- PMCID: PMC8482841
- DOI: 10.3389/fnagi.2021.621023
A Multimodal Risk Network Predicts Executive Function Trajectories in Non-demented Aging
Abstract
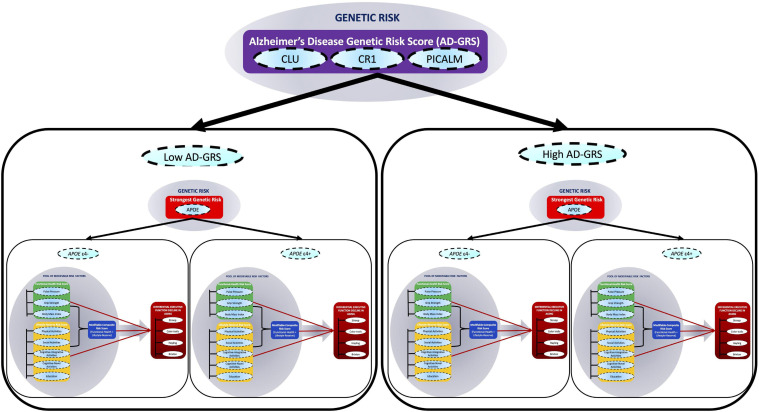
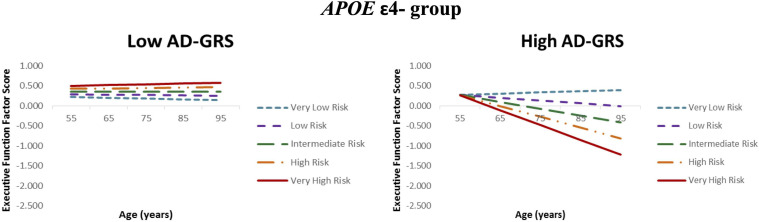
Background: Multiple modalities of Alzheimer's disease (AD) risk factors may operate through interacting networks to predict differential cognitive trajectories in asymptomatic aging. We test such a network in a series of three analytic steps. First, we test independent associations between three risk scores (functional-health, lifestyle-reserve, and a combined multimodal risk score) and cognitive [executive function (EF)] trajectories. Second, we test whether all three associations are moderated by the most penetrant AD genetic risk [Apolipoprotein E (APOE) ε4+ allele]. Third, we test whether a non-APOE AD genetic risk score further moderates these APOE × multimodal risk score associations. Methods: We assembled a longitudinal data set (spanning a 40-year band of aging, 53-95 years) with non-demented older adults (baseline n = 602; Mage = 70.63(8.70) years; 66% female) from the Victoria Longitudinal Study (VLS). The measures included for each modifiable risk score were: (1) functional-health [pulse pressure (PP), grip strength, and body mass index], (2) lifestyle-reserve (physical, social, cognitive-integrative, cognitive-novel activities, and education), and (3) the combination of functional-health and lifestyle-reserve risk scores. Two AD genetic risk markers included (1) APOE and (2) a combined AD-genetic risk score (AD-GRS) comprised of three single nucleotide polymorphisms (SNPs; Clusterin[rs11136000], Complement receptor 1[rs6656401], Phosphatidylinositol binding clathrin assembly protein[rs3851179]). The analytics included confirmatory factor analysis (CFA), longitudinal invariance testing, and latent growth curve modeling. Structural path analyses were deployed to test and compare prediction models for EF performance and change. Results: First, separate analyses showed that higher functional-health risk scores, lifestyle-reserve risk scores, and the combined score, predicted poorer EF performance and steeper decline. Second, APOE and AD-GRS moderated the association between functional-health risk score and the combined risk score, on EF performance and change. Specifically, only older adults in the APOEε4- group showed steeper EF decline with high risk scores on both functional-health and combined risk score. Both associations were further magnified for adults with high AD-GRS. Conclusion: The present multimodal AD risk network approach incorporated both modifiable and genetic risk scores to predict EF trajectories. The results add an additional degree of precision to risk profile calculations for asymptomatic aging populations.
Keywords: Alzheimer’s disease; Victoria Longitudinal Study; cognitive trajectories; genetic risk scores; modifiable risk factors; normal aging.
Copyright © 2021 Sapkota, McFall, Masellis and Dixon.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A Network of Genetic Effects on Non-Demented Cognitive Aging: Alzheimer's Genetic Risk (CLU + CR1 + PICALM) Intensifies Cognitive Aging Genetic Risk (COMT + BDNF) Selectively for APOEɛ4 Carriers.J Alzheimers Dis. 2018;62(2):887-900. doi: 10.3233/JAD-170909. J Alzheimers Dis. 2018. PMID: 29480189 Free PMC article.
-
Alzheimer's Disease Biomarkers Interactively Influence Physical Activity, Mobility, and Cognition Associations in a Non-Demented Aging Population.J Alzheimers Dis. 2017;60(1):69-86. doi: 10.3233/JAD-170130. J Alzheimers Dis. 2017. PMID: 28800331
-
Physical Activity and Mobility Differentially Predict Nondemented Executive Function Trajectories: Do Sex and APOE Moderate These Associations?Gerontology. 2019;65(6):640-648. doi: 10.1159/000496442. Epub 2019 Mar 25. Gerontology. 2019. PMID: 30909272
-
Differential Cognitive Decline in Alzheimer's Disease Is Predicted by Changes in Ventricular Size but Moderated by Apolipoprotein E and Pulse Pressure.J Alzheimers Dis. 2022;85(2):545-560. doi: 10.3233/JAD-215068. J Alzheimers Dis. 2022. PMID: 34864669
-
Understanding disease progression and improving Alzheimer's disease clinical trials: Recent highlights from the Alzheimer's Disease Neuroimaging Initiative.Alzheimers Dement. 2019 Jan;15(1):106-152. doi: 10.1016/j.jalz.2018.08.005. Epub 2018 Oct 13. Alzheimers Dement. 2019. PMID: 30321505 Review.
Cited by
-
Vascular Risk Predicts Plasma Amyloid β 42/40 Through Cerebral Amyloid Burden in Apolipoprotein E ε4 Carriers.Stroke. 2023 May;54(5):1227-1235. doi: 10.1161/STROKEAHA.122.041854. Epub 2023 Apr 6. Stroke. 2023. PMID: 37021572 Free PMC article.
-
Brain atrophy trajectories predict differential functional performance in Alzheimer's disease: Moderations with apolipoprotein E and sex.Alzheimers Dement (Amst). 2021 Oct 14;13(1):e12244. doi: 10.1002/dad2.12244. eCollection 2021. Alzheimers Dement (Amst). 2021. PMID: 34692981 Free PMC article.
References
-
- Albanese E., Launer L. J., Egger M., Prince M. J., Giannakopoulos P., Wolters F. J., et al. (2017). Body mass index in midlife and dementia: systematic review and meta-regression analysis of 589,649 men and women followed in longitudinal studies. Alzheimer’s Dement. Diagnosis, Assess. Dis. Monit. 8 165–178. 10.1016/j.dadm.2017.05.007 - DOI - PMC - PubMed
-
- Andrews S. J., McFall G. P., Dixon R. A., Cherbuin N., Eramudugolla R., Anstey K. J. (2019). Alzheimer’s environmental and genetic risk scores are differentially associated with general cognitive ability and dementia severity. Alzheimer Dis. Assoc. Disord. 33 95–103. 10.1097/WAD.0000000000000292 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous