

Cholera risk in cities in Uganda: understanding cases and contacts centered strategy (3CS) for rapid cholera outbreak control
- PMID: 34603574
- PMCID: PMC8464210
- DOI: 10.11604/pamj.2021.39.193.27794
Cholera risk in cities in Uganda: understanding cases and contacts centered strategy (3CS) for rapid cholera outbreak control
Abstract
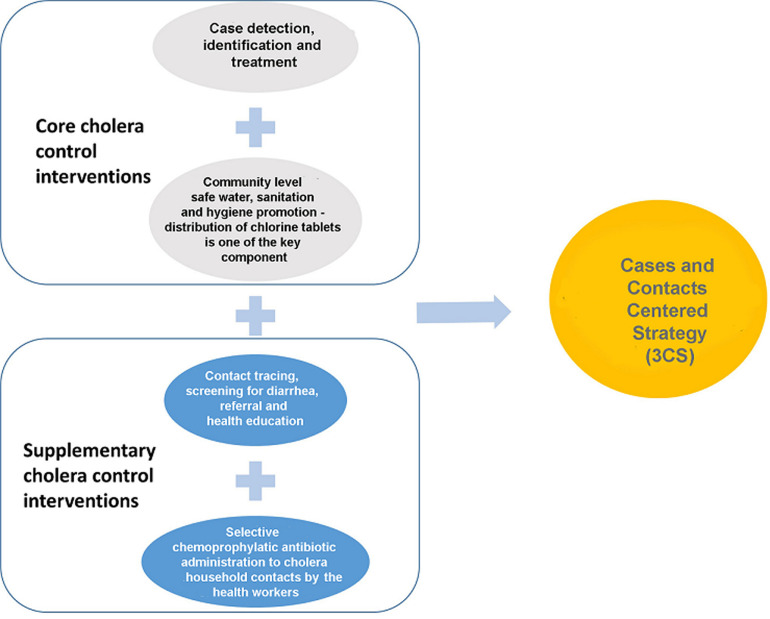
Introduction: in the recent past, cities in sub-Saharan Africa have reported serious cholera outbreaks that last for several months. Uganda is one of the African countries where cities are prone to cholera outbreaks. Studies on cholera in Bangladesh show increased risk of cholera for the immediate household members (contacts) yet the control interventions mainly target cases with little or no focus on contacts. This study aimed to describe the rapid control of cholera outbreaks in Kampala and Mbale cities, Uganda, using, "Cases and Contacts Centered Strategy (3CS)" that consisted of identification and treatment of cases, promotion of safe water, sanitation, hygiene (WaSH) and selective chemoprophylaxis for the contacts.
Methods: a cross-sectional study was conducted in 2015-2016 in the Kampala and Mbale cities during cholera outbreaks. Cholera cases were treated and 816 contacts from 188 households were listed and given cholera preventive packages. Data were collected, cleaned, analysed and stored in spreadsheet. Comparison of categories was done using Chi-Square test.
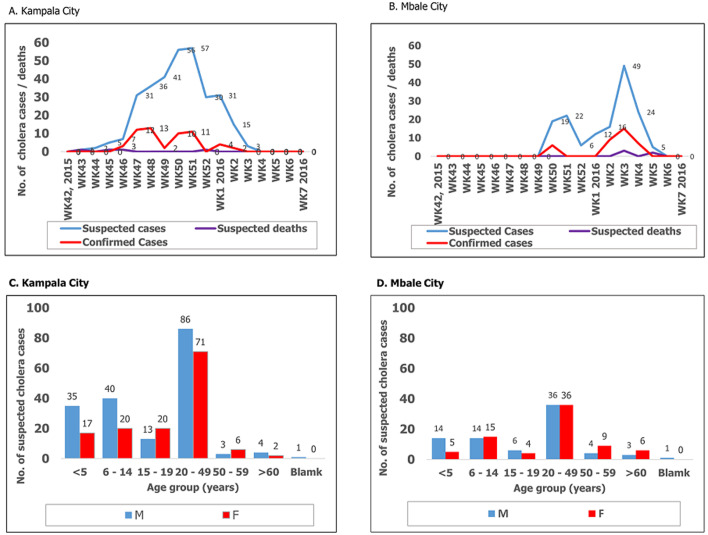
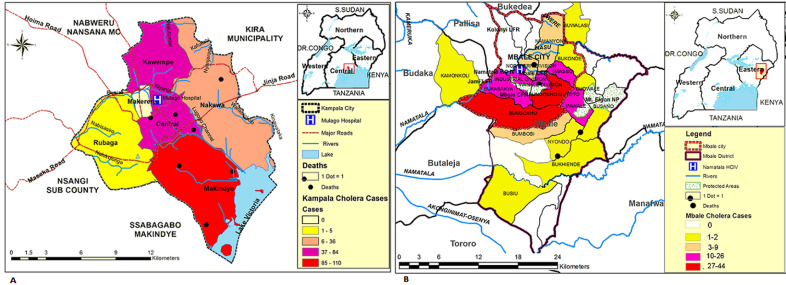
Results: a total of 58 and 41 confirmed cholera cases out of 318 and 153 suspected cases were recorded in Kampala and Mbale cities respectively. The outbreaks lasted for 41 days in both cities. Case fatality rates were high; 12.1% (5/41) for Mbale city and 1.7% (1/58) for Kampala city. Fifty-five percent (210/379) of stool samples were tested by culture to confirm V. choleraeO1. No contacts listed and given cholera preventive package developed cholera. Both sexes and all age groups were affected. In Kampala city, the males were more affected than the females in the age groups less than 14 years, p-value of 0.0097.
Conclusion: this study showed that by implementing 3CS, it was possible to rapidly control cholera outbreaks in Kampala and Mbale cities and no cholera cases were reported amongst the listed household contacts. The findings on 3CS and specifically, selective antibiotic chemoprophylaxis for cholera prevention, could be used in similar manner to oral cholera vaccines to complement the core cholera control interventions (disease surveillance, treatment of cases and WaSH). However, studies are needed to guide such rollout and to understand the age-sex differences in Kampala city.
Keywords: Africa; Cholera; Kampala; Uganda; chemoprophylaxis; city; infection; outbreak; prevention; treatment.
Copyright: Godfrey Bwire et al.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
