

Ambulatory monitoring promises equitable personalized healthcare delivery in underrepresented patients
- PMID: 34604759
- PMCID: PMC8482046
- DOI: 10.1093/ehjdh/ztab047
Ambulatory monitoring promises equitable personalized healthcare delivery in underrepresented patients
Abstract
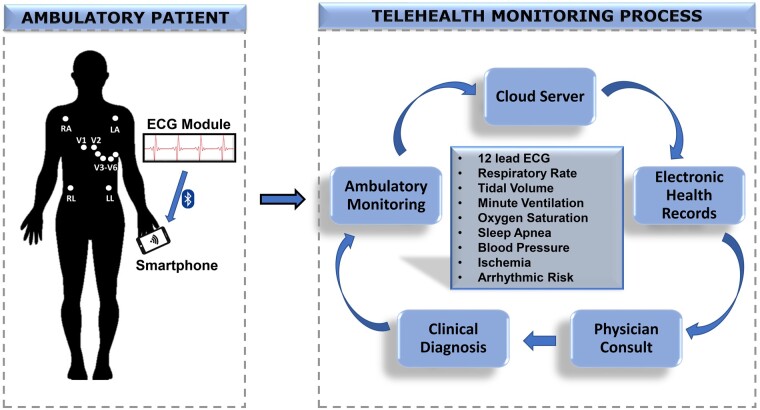
The pandemic has brought to everybody's attention the apparent need of remote monitoring, highlighting hitherto unseen challenges in healthcare. Today, mobile monitoring and real-time data collection, processing and decision-making, can drastically improve the cardiorespiratory-haemodynamic health diagnosis and care, not only in the rural communities, but urban ones with limited healthcare access as well. Disparities in socioeconomic status and geographic variances resulting in regional inequity in access to healthcare delivery, and significant differences in mortality rates between rural and urban communities have been a growing concern. Evolution of wireless devices and smartphones has initiated a new era in medicine. Mobile health technologies have a promising role in equitable delivery of personalized medicine and are becoming essential components in the delivery of healthcare to patients with limited access to in-hospital services. Yet, the utility of portable health monitoring devices has been suboptimal due to the lack of user-friendly and computationally efficient physiological data collection and analysis platforms. We present a comprehensive review of the current cardiac, pulmonary, and haemodynamic telemonitoring technologies. We also propose a novel low-cost smartphone-based system capable of providing complete cardiorespiratory assessment using a single platform for arrhythmia prediction along with detection of underlying ischaemia and sleep apnoea; we believe this system holds significant potential in aiding the diagnosis and treatment of cardiorespiratory diseases, particularly in underserved populations.
Keywords: Cardiorespiratory; Haemodynamic; Monitoring; Personalized medicine; Smartphone; Telehealth.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures






References
-
- Pew research internet project. Mobile technology fact sheet. 2014. http://www.Pewinternet.Org/fact-sheets/mobile-technology-fact-sheet (11 ....
-
- Nigam G, Pathak C, Riaz M.. A systematic review of central sleep apnea in adult patients with chronic kidney disease. Sleep Breath 2016;20:957–964. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources